Department of Pathology and Laboratory Medicine, The Children's Hospital of Philadelphia, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, PA, USA.
Department of Pathology and Laboratory Medicine, Hospital of the University of Pennsylvania, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, PA, USA.
Mod Pathol. 2022 Dec;35(12):1870-1881. doi: 10.1038/s41379-022-01129-0. Epub 2022 Jul 6.
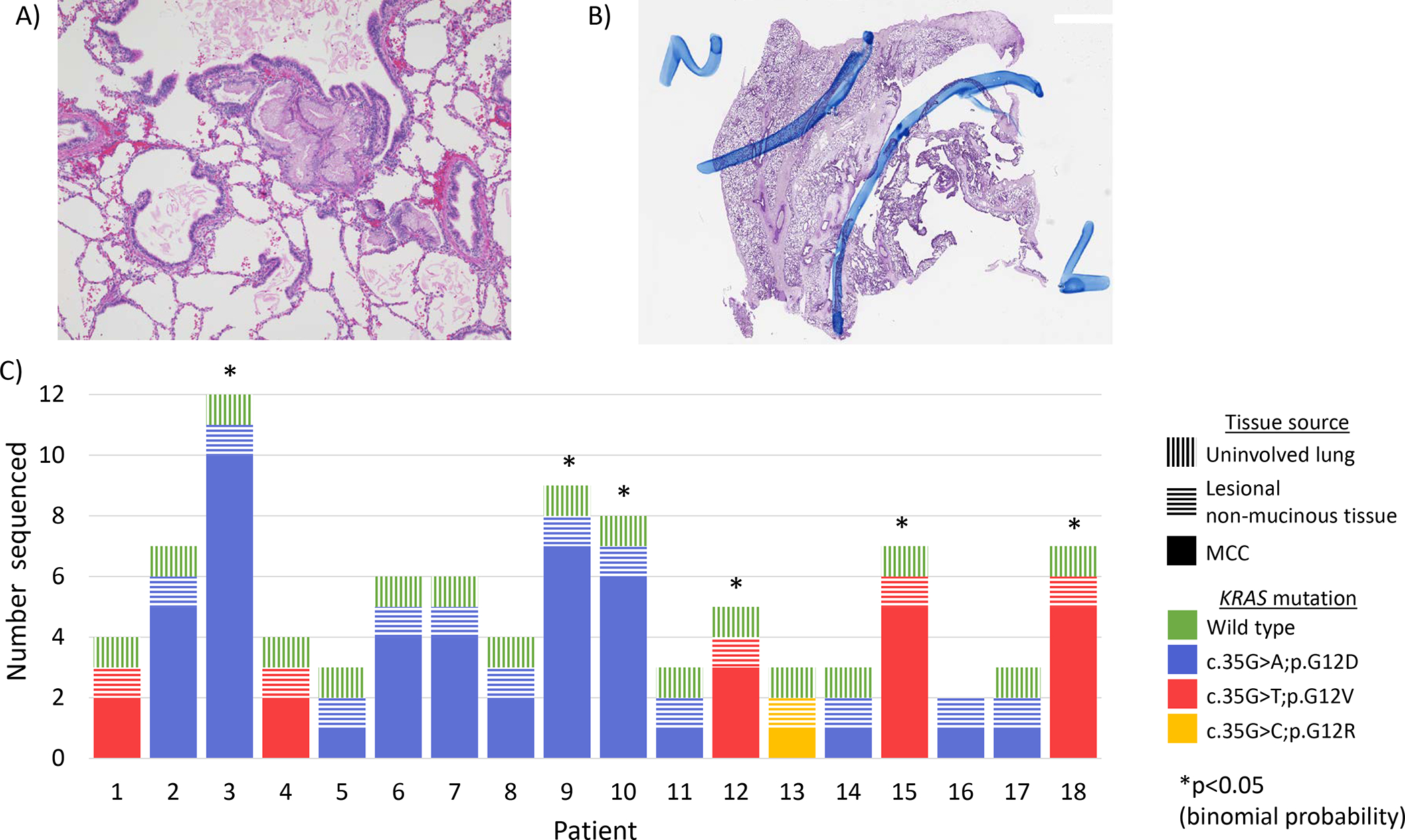
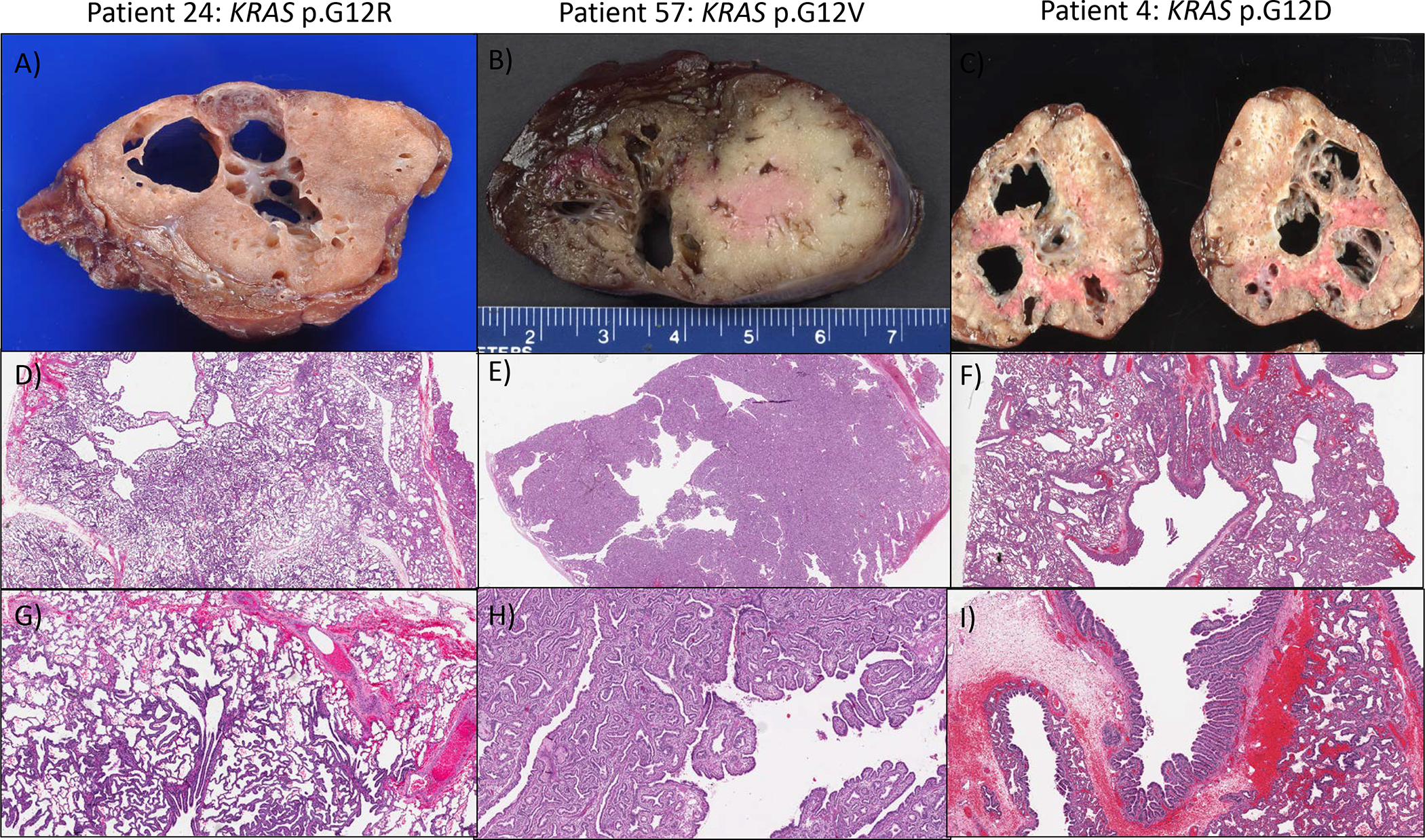
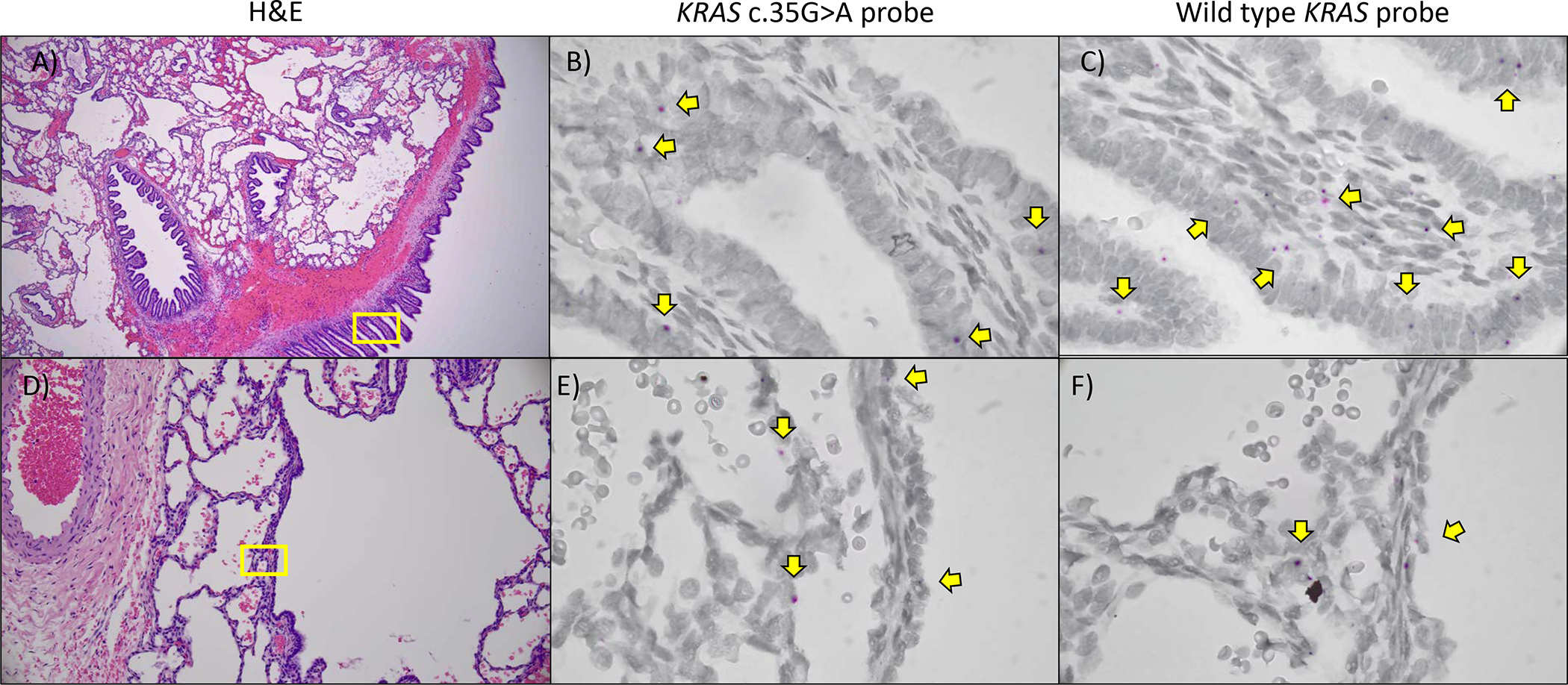
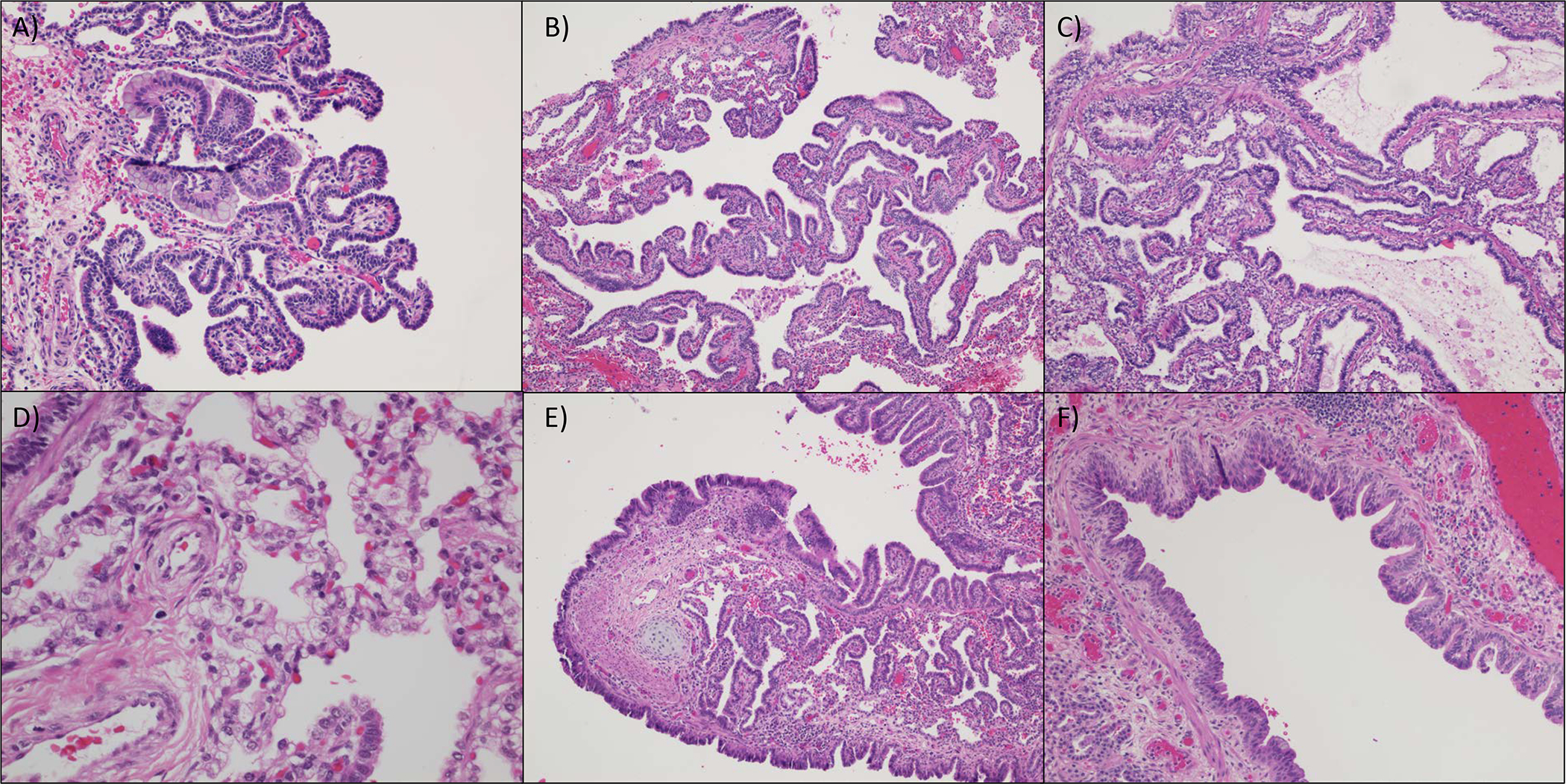
The potential pathogenetic mechanisms underlying the varied morphology of congenital pulmonary airway malformations (CPAMs) have not been molecularly determined, but a subset have been shown to contain clusters of mucinous cells (MCC). These clusters are believed to serve as precursors for potential invasive mucinous adenocarcinoma, and they are associated with KRAS codon 12 mutations. To assess the universality of KRAS mutations in MCCs, we sequenced exon 2 of KRAS in 61 MCCs from 18 patients, and we found a KRAS codon 12 mutation in all 61 MCCs. Furthermore, all MCCs from a single patient always had the same KRAS mutation, and the same KRAS mutation was also found in non-mucinous lesional tissue. Next generation sequencing of seven MCCs showed no other mutations or copy number variations. Sequencing of 46 additional CPAMs with MCCs revealed KRAS mutations in non-mucinous lesional tissue in all cases. RNA in situ hybridization confirmed widespread distribution of cells with mutant KRAS RNA, even extending outside of the bronchiolar type epithelium. We identified 25 additional CPAMs with overall histologic architecture similar to CPAMs with KRAS mutations but without identifiable MCCs, and we found KRAS mutations in 17 (68%). The histologic features of these KRAS mutated CPAMs included type 1 and type 3 morphology, as well as lesions with an intermediate histologic appearance, and analysis revealed a strong correlation between the specific amino acid substitution and histomorphology. These findings, together with previously published model organism data, suggests that the formation of type 1 and 3 CPAMs is driven by mosaic KRAS mutations arising in the lung epithelium early in development and places them within the growing field of mosaic RASopathies. The presence of widespread epithelial mutation explains late metastatic disease in incompletely resected patients and reinforces the recommendation for complete resection of these lesions.
先天性肺气道畸形(CPAMs)形态多样的潜在发病机制尚未从分子水平确定,但有一部分已被证明含有黏液细胞簇(MCC)。这些簇被认为是潜在侵袭性黏液性腺癌的前体,并且与 KRAS 密码子 12 突变有关。为了评估 MCC 中 KRAS 突变的普遍性,我们对 18 名患者的 61 个 MCC 进行了 KRAS 外显子 2 的测序,发现所有 61 个 MCC 均存在 KRAS 密码子 12 突变。此外,单个患者的所有 MCC 总是具有相同的 KRAS 突变,并且在非黏液性病变组织中也发现了相同的 KRAS 突变。对七个 MCC 进行下一代测序显示,没有其他突变或拷贝数变异。对另外 46 个伴有 MCC 的 CPAMs 进行测序,发现所有病例的非黏液性病变组织中均存在 KRAS 突变。RNA 原位杂交证实,存在突变 KRAS RNA 的细胞广泛分布,甚至延伸到细支气管型上皮之外。我们确定了另外 25 个 CPAMs,其总体组织学结构与具有 KRAS 突变的 CPAMs 相似,但没有可识别的 MCC,并且在 17 个(68%)中发现了 KRAS 突变。这些 KRAS 突变 CPAMs 的组织学特征包括 1 型和 3 型形态,以及具有中间组织学表现的病变,并且分析显示特定氨基酸取代与组织形态学之间存在很强的相关性。这些发现,以及以前发表的模式生物数据,表明 1 型和 3 型 CPAMs 的形成是由肺上皮细胞在早期发育过程中发生的镶嵌性 KRAS 突变驱动的,并将它们置于不断发展的镶嵌性 RAS 病变领域内。广泛的上皮突变的存在解释了不完全切除患者中晚期转移性疾病的发生,并强化了对这些病变进行完全切除的建议。