Department of Anesthesiology, Qilu Hospital of Shangdong University, 107 Wenhua Xi Road, Jinan, 250012, Shandong, China.
Department of Anesthesiology, Critical Care and Pain Medicine, Beth Israel Deaconess Medical Center, 330 Brookline Avenue, Boston, MA, 02215, USA.
BMC Anesthesiol. 2022 Jul 6;22(1):208. doi: 10.1186/s12871-022-01753-y.
Either neuraxial anesthesia or general anesthesia can be performed for cesarean delivery. Generally, neuraxial anesthesia is the first choice with the risk and benefit balance for both the mother and fetus. However, general anesthesia is also applicable most commonly in the emergent setting. This study analyzed maternal complications associated with general anesthesia for cesarean delivery and suggested lowering pregnancy-related maternal and newborn adverse outcomes.
With the approval of the Institutional Ethics Review Board (No: 2017016), data on cesarean delivery and related anesthesia were collected from the Electronic Health Record System from 1/1/2013 to 12/31/2016. Statistical software STATA version 15.1 was used for data analyses. All statistical tests were two-sided, and a level significance of 0.05 was assumed.
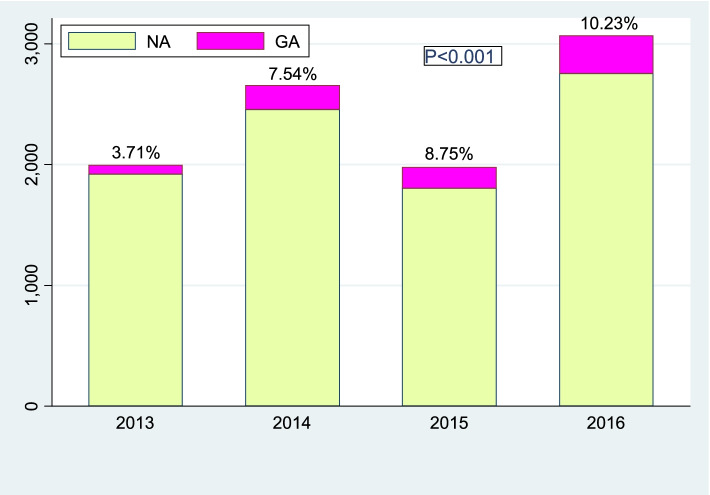
The rate of general anesthesia for cesarean delivery increased steadily during 2013-2016, 3.71% in 2013 to 10.23% in 2016 (p < 0.001). Repeat cesarean delivery among general anesthesia group increased significantly from 16.22% in 2013 to 54.14% in 2016 (p < 0.001). Morbidly adherent placenta (MAP) was the first reason among pregnancy-related complications, which accounted for 33% in total in general anesthesia group (38% in 2013 to 44% in 2016). The laryngeal mask airway (LMA) was used in airway management, and the proportion of LMA increased from 28.38% in 2013 to 92.99% in 2016 (p < 0.001). There were significant differences in newborn outcomes between general anesthesia and neuraxial anesthesia groups, including newborn weight, newborn Apgar score at 1 min and 5 min and newborn admission to the NICU (p < 0.001).
The growing incidence of general anesthesia was consistent with the trend of rising repeat cesarean delivery and MAP. low newborn Apgar score and high newborn admission to the NICU in general anesthesia group compared with neuraxial anesthesia group. The LMA was performed safely for airway management with enough fasting and careful gastric volume evaluation.
剖宫产术可以选择椎管内麻醉或全身麻醉。通常情况下,椎管内麻醉是首选,以实现母婴风险与获益的平衡。然而,全身麻醉在紧急情况下也很常用。本研究分析了全身麻醉行剖宫产术相关的母体并发症,并建议降低与妊娠相关的母婴不良结局。
本研究经机构伦理审查委员会批准(编号:2017016),从电子健康记录系统中收集了 2013 年 1 月 1 日至 2016 年 12 月 31 日的剖宫产术和相关麻醉数据。采用统计软件 STATA 版本 15.1 进行数据分析。所有统计检验均为双侧检验,显著性水平设为 0.05。
2013 年至 2016 年,全身麻醉行剖宫产术的比例稳步上升,从 2013 年的 3.71%上升至 2016 年的 10.23%(p<0.001)。全身麻醉组的再次剖宫产率从 2013 年的 16.22%显著增加至 2016 年的 54.14%(p<0.001)。与妊娠相关的并发症中,胎盘粘连(MAP)是首要原因,占全身麻醉组的 33%(2013 年为 38%,2016 年为 44%)。在气道管理中使用喉罩气道(LMA),LMA 的比例从 2013 年的 28.38%上升至 2016 年的 92.99%(p<0.001)。全身麻醉组与椎管内麻醉组新生儿结局存在显著差异,包括新生儿体重、1 分钟和 5 分钟新生儿 Apgar 评分以及新生儿入住新生儿重症监护病房(NICU)(p<0.001)。
全身麻醉发生率的增加与再次剖宫产术和 MAP 发生率的上升趋势一致。与椎管内麻醉组相比,全身麻醉组新生儿 Apgar 评分较低,新生儿入住 NICU 比例较高。在充分禁食和仔细评估胃容量的情况下,LMA 可安全用于气道管理。