Dave Chintan, Sivajohan Asaanth, Basmaji John, Slessarev Marat
Department of Medicine, Division of Critical Care, Western University, London, ON.
Schulich School of Medicine & Dentistry, Western University, London, ON.
Crit Care Explor. 2022 Jun 30;4(7):e0723. doi: 10.1097/CCE.0000000000000723. eCollection 2022 Jul.
To inform the design of open-source ventilators, we performed a systematic review of clinical practice guidelines (CPGs) to consolidate the evidence on mechanical ventilation strategies that result in improved patient-important outcomes for acute hypoxic respiratory failure.
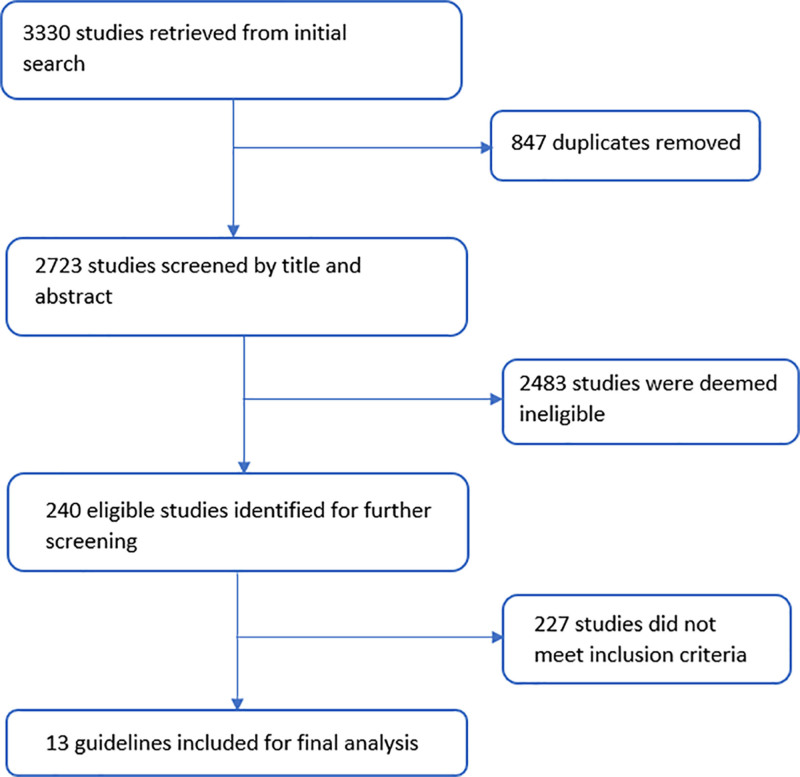
We developed a search strategy to identify relevant CPGs from Ovid Medline, Ovid Medline In-Process & Other Non-Indexed Citations, Embase, the Cochrane Library, Mendeley, and Google scholar from 2010 to February 17, 2022.
Using a two-step screening process with two independent reviewers, we included CPGs that made recommendations on mechanical ventilation strategies of interest. Guidelines that reported at least one recommendation about mechanical ventilation in ICU patients with acute hypoxic respiratory failure were included.
From the 13 eligible guidelines, we collected data on country, aim, patient population, impact on morbidity and mortality (effect size and CIs), recommendations, strength of Recommendation (as per Grading of Recommendations, Assessment, Development and Evaluations), and details of supporting evidence base.
We identified three ventilation strategies that confer a mortality and morbidity benefit for ventilated patients with acute hypoxic respiratory failure: low-tidal volume ventilation, plateau pressures of less than 30 cm HO, and higher positive end-expiratory pressure (PEEP). These moderate-to-strong recommendations were based on moderate-to-high certainty in evidence. We identified several other recommendations with no or minimal certainty in evidence.
Our systematic review of international CPGs identified no recommendations favoring specific mode of ventilation and three ventilation strategies that confer mortality and morbidity benefits, backed by moderate-to-strong evidence. Ventilator design teams must include the ability to consistently provide and measure low-tidal volume ventilation, plateau pressures of less than 30 cm HO, and higher PEEP into their designs. Based on our findings, we provide the first public framework for open-source ventilator design.
为指导开源呼吸机的设计,我们对临床实践指南(CPG)进行了系统评价,以整合关于机械通气策略的证据,这些策略能改善急性低氧性呼吸衰竭患者的重要预后。
我们制定了检索策略,以识别2010年至2022年2月17日期间来自Ovid Medline、Ovid Medline在研及其他未索引引文、Embase、Cochrane图书馆、Mendeley和谷歌学术的相关CPG。
通过两名独立评审员的两步筛选过程,我们纳入了对感兴趣的机械通气策略提出建议的CPG。纳入了报告了至少一项关于急性低氧性呼吸衰竭ICU患者机械通气建议的指南。
从13项符合条件的指南中,我们收集了关于国家、目的、患者群体、对发病率和死亡率的影响(效应大小和置信区间)、建议、推荐强度(根据推荐分级、评估、制定和评价)以及支持证据基础细节的数据。
我们确定了三种通气策略,对急性低氧性呼吸衰竭的通气患者具有降低死亡率和发病率的益处:低潮气量通气、平台压小于30 cm H₂O以及较高的呼气末正压(PEEP)。这些中等到强烈建议基于证据的中等到高度确定性。我们还确定了其他一些证据确定性低或无的建议。
我们对国际CPG的系统评价未发现支持特定通气模式的建议,而是确定了三种具有降低死亡率和发病率益处的通气策略,并有中等到强有力的证据支持。呼吸机设计团队必须在其设计中纳入持续提供和测量低潮气量通气、平台压小于30 cm H₂O以及较高PEEP的能力。基于我们的研究结果,我们提供了首个开源呼吸机设计的公共框架。