Allergy Immunology Unit, Department of Pediatrics, Advanced Pediatrics Centre, Post Graduate Institute of Medical Education and Research, Chandigarh, India.
Front Immunol. 2022 Jun 20;13:869466. doi: 10.3389/fimmu.2022.869466. eCollection 2022.
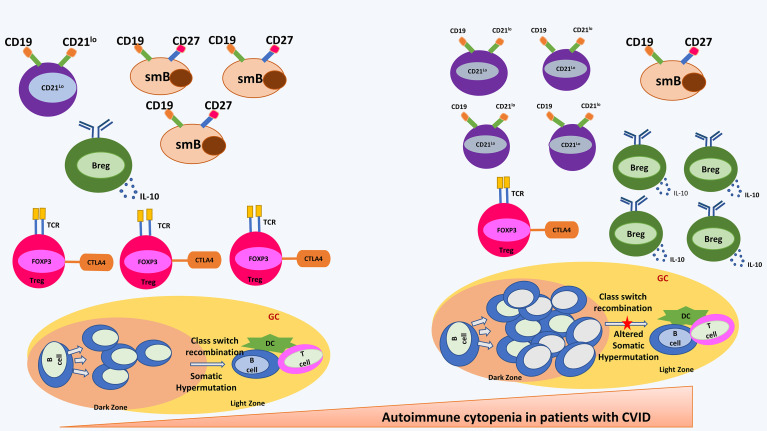
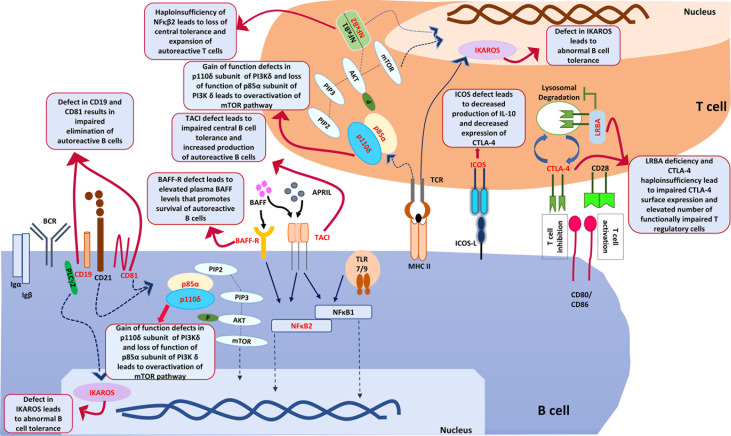
Common variable immunodeficiency (CVID) is the most common symptomatic primary immunodeficiency (PID). CVID is a heterogenous condition and clinical manifestations may vary from increased susceptibility to infections to autoimmune manifestations, granulomatous disease, polyclonal lymphoproliferation, and increased risk of malignancy. Autoimmune manifestations may, at times, be the first and only clinical presentation of CVID, resulting in diagnostic dilemma for the treating physician. Autoimmune cytopenias (autoimmune haemolytic anaemia and/or thrombocytopenia) are the most common autoimmune complications seen in patients with CVID. Laboratory investigations such as antinuclear antibodies, direct Coomb's test and anti-platelet antibodies may not be useful in patients with CVID because of lack of specific antibody response. Moreover, presence of autoimmune cytopenias may pose a significant therapeutic challenge as use of immunosuppressive agents can be contentious in these circumstances. It has been suggested that serum immunoglobulins must be checked in all patients presenting with autoimmune cytopenia such as immune thrombocytopenia or autoimmune haemolytic anaemia. It has been observed that patients with CVID and autoimmune cytopenias have a different clinical and immunological profile as compared to patients with CVID who do not have an autoimmune footprint. Monogenic defects have been identified in 10-50% of all patients with CVID depending upon the population studied. Monogenic defects are more likely to be identified in patients with CVID with autoimmune complications. Common genetic defects that may lead to CVID with an autoimmune phenotype include and In this review, we update on recent advances in pathophysiology and management of CVID with autoimmune cytopenias.
普通变异性免疫缺陷(CVID)是最常见的有症状原发性免疫缺陷(PID)。CVID 是一种异质性疾病,临床表现可从易感染到自身免疫表现、肉芽肿病、多克隆淋巴增生和恶性肿瘤风险增加不等。自身免疫表现有时可能是 CVID 的首发和唯一临床表现,导致治疗医生面临诊断难题。自身免疫性细胞减少症(自身免疫性溶血性贫血和/或血小板减少症)是 CVID 患者最常见的自身免疫并发症。由于缺乏特异性抗体反应,核抗体、直接 Coomb 试验和抗血小板抗体等实验室检查在 CVID 患者中可能没有用处。此外,自身免疫性细胞减少症的存在可能会带来重大的治疗挑战,因为在这种情况下使用免疫抑制剂可能存在争议。有人建议,所有出现自身免疫性细胞减少症(如免疫性血小板减少症或自身免疫性溶血性贫血)的患者都应检查血清免疫球蛋白。人们观察到,与没有自身免疫足迹的 CVID 患者相比,患有 CVID 和自身免疫性细胞减少症的患者具有不同的临床和免疫学特征。根据研究的人群,在所有 CVID 患者中,有 10-50%的患者发现了单基因缺陷。有自身免疫并发症的 CVID 患者更有可能发现单基因缺陷。可能导致具有自身免疫表型的 CVID 的常见遗传缺陷包括 和 。在这篇综述中,我们更新了 CVID 伴自身免疫性细胞减少症的发病机制和治疗的最新进展。