Joshi Nehal, Lango-Allen Hana, Downes Kate, Simeoni Ilenia, Vladescu Camelia, Paul Deena, Hart Alice, Ademokun Christine, Cooper Nichola
Centre for Haematology, Department of Immunology and Inflammation, Imperial College London, London, United Kingdom.
Department of Haematology, University of Cambridge, Cambridge Biomedical Campus, Cambridge, United Kingdom.
Blood Adv. 2025 Apr 8;9(7):1497-1507. doi: 10.1182/bloodadvances.2024014639.
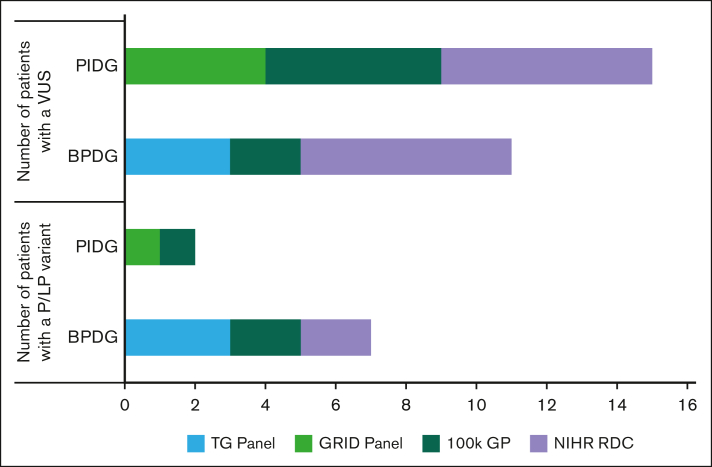
Immune thrombocytopenia (ITP) is a heterogenous autoimmune disorder diagnosed by excluding other conditions. Misdiagnosis of primary ITP occurs in patients with inherited thrombocytopenia and primary immunodeficiency syndromes. This study investigates whether genetic testing for inherited thrombocytopenia or primary immunodeficiency can enhance diagnostic accuracy in ITP, and guide treatment strategies. We performed whole genome sequencing or targeted panel sequencing on peripheral blood samples in a cohort of 80 participants with chronic ITP, utilizing the ThromboGenomics panel (n = 72) and the Genomics of Rare Immune Disorders panel (n = 50) consisting of genes known to cause bleeding and platelet disorders (BPDG) or primary immuodeficiency genes (PIDG) respectively. A replication cohort of 73 patients underwent clinical genomics testing with either the R90 (BPDG, n = 35) or R15 (PIDG, n = 50) National Health Service Genomics panels. Known pathogenic or likely pathogenic, disease-causing, variants were identified in 9 patients in the first cohort (11%, 95% confidence interval [CI]: 5-20); 7 patients (10%, 95% CI: 4-19) in BPDG and 2 patients (4% CI,1-14) in PIDG. In addition, 26 patients (32.5%) carried variants of uncertain significance. In the replication cohort, 8% (95% CI, 2-20) and 9% (95% CI, 2-23) of patients had a pathogenic variant identified on the R15 (PIDG) or R90 panel (BPDG), respectively. The findings impacted clinical management such as avoidance of immunosuppression (ANKRD26, GP1BB, ETV6, TUBB1, and ITGB3) and eligibility for allogeneic stem cell transplantation (UNC13D). Our findings demonstrate that genomic sequencing identifies diagnostically relevant variants in patients with chronic ITP. Identification of these variants can guide treatment decisions and improve patient outcomes.
免疫性血小板减少症(ITP)是一种异质性自身免疫性疾病,通过排除其他病症来诊断。原发性ITP的误诊发生在遗传性血小板减少症和原发性免疫缺陷综合征患者中。本研究调查遗传性血小板减少症或原发性免疫缺陷的基因检测是否能提高ITP的诊断准确性,并指导治疗策略。我们对80名慢性ITP参与者的外周血样本进行了全基因组测序或靶向基因panel测序,使用了血栓基因组学panel(n = 72)和罕见免疫疾病基因组学panel(n = 50),分别由已知导致出血和血小板疾病(BPDG)或原发性免疫缺陷基因(PIDG)的基因组成。73名患者的复制队列接受了使用R90(BPDG,n = 35)或R15(PIDG,n = 50)英国国家医疗服务体系基因组panel的临床基因组学检测。在第一个队列中,9名患者(11%,95%置信区间[CI]:5 - 20)鉴定出已知的致病或可能致病的致病变体;BPDG中有7名患者(10%,95% CI:4 - 19),PIDG中有2名患者(4% CI,1 - 14)。此外,26名患者(32.5%)携带意义未明的变体。在复制队列中,分别有8%(95% CI,2 - 20)和9%(95% CI,2 - 23)的患者在R15(PIDG)或R90 panel(BPDG)上鉴定出致病变体。这些发现影响了临床管理,如避免免疫抑制(ANKRD26、GP1BB、ETV6、TUBB1和ITGB3)以及异基因干细胞移植的适用性(UNC13D)。我们的研究结果表明,基因组测序可在慢性ITP患者中鉴定出与诊断相关的变体。鉴定这些变体可指导治疗决策并改善患者预后。