Pissarra Rita, Pereira Marisa, Amorim Rita, Neto Bárbara Pereira, Lourenço Lara, Santos Luís Almeida
Pediatrics Department.
Pediatric Emergency Department, Centro Hospitalar Universitário São João, Porto, Portugal.
Porto Biomed J. 2022 Jun 17;7(3):e150. doi: 10.1097/j.pbj.0000000000000150. eCollection 2022 May-Jun.
Chest pain in children and adolescents is a common complaint in the emergency department (ED), being mostly benign. A thorough patient history and physical examination should be enough in most cases for its proper management. Regarding non-cardiac chest pain, anxiety plays an important role.
Retrospective analysis of all admissions in a pediatric ED of a Portuguese third-level hospital with a chief complaint of chest pain between January and December 2018. Chi-square test was used to compare different etiologies, considering a significance level of 5%.
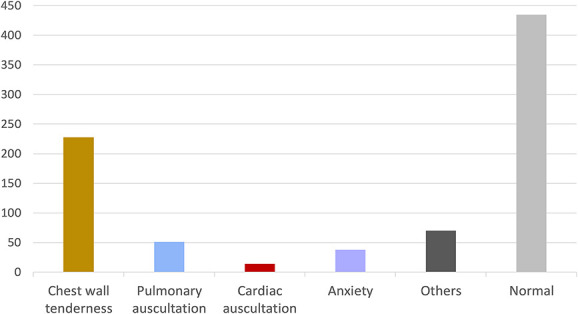
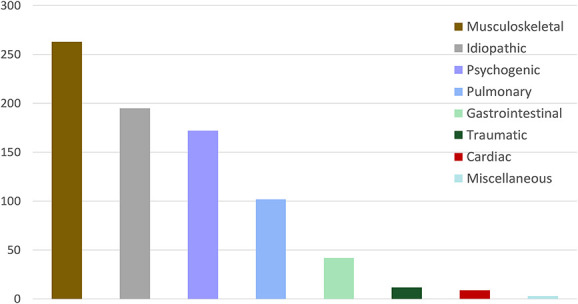
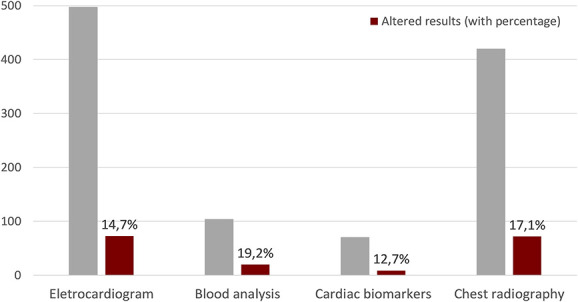
A total of 798 visits were included: 53.6% girls, 80.8% adolescents (mean age: 13years old). According to the Pediatric Canadian Triage and Acuity Scale, 77.7% was prioritized as level IV: less urgent; 65.3% reported associated symptoms including dyspnea (31.8%), cough (18.2%), and palpitations (16.1%). In physical examination, 45.5% had alterations: 62.8% with chest wall tenderness. Further investigation was done in 84% of patients: 62.4% electrocardiograms (altered in 14.7%), 52.6% chest radiographies (altered in 17.1%) and 8.9% cardiac biomarkers (altered in 12.7%). The 3 main causes of chest pain were musculoskeletal (33%), idiopathic (24.4%) and psychogenic (21.6%), with 1.1% of cardiac etiology. Less than 3% needed hospital admission and 18.9% were oriented to an outpatient consultation. 7.1% readmissions reported. When compared to other causes as a group, psychogenic chest pain presented a statistically significant association with female sex, adolescence, psychiatric antecedents, previous stressful event, and normal physical examination. Of these, <30% were oriented to a pedopsychiatry/psychology consultation.
Opposing to the low priority level in triage, benign diagnosis found, and low hospital admissions, there was a high percentage of complementary diagnostic tests performed with few altered results. In psychogenic chest pain there was a low postdischarge referral. The authors highlight the importance of clinical algorithms to reduce unnecessary tests performed and readmissions and improve orientation and follow-up, particularly in psychogenic etiology.
儿童和青少年胸痛是急诊科常见的主诉,大多为良性。在大多数情况下,详尽的病史和体格检查足以对其进行妥善处理。对于非心源性胸痛,焦虑起着重要作用。
对葡萄牙一家三级医院儿科急诊科2018年1月至12月期间以胸痛为主诉的所有住院病例进行回顾性分析。采用卡方检验比较不同病因,显著性水平为5%。
共纳入798例就诊病例:女孩占53.6%,青少年占80.8%(平均年龄:13岁)。根据加拿大儿科分诊和 acuity 量表,77.7%被列为IV级:不太紧急;65.3%报告有相关症状,包括呼吸困难(31.8%)、咳嗽(18.2%)和心悸(16.1%)。体格检查中,45.5%有异常:62.8%有胸壁压痛感。84%的患者进行了进一步检查:62.4%做了心电图(14.7%有异常),52.6%做了胸部X光检查(17.1%有异常),8.9%检测了心脏生物标志物(12.7%有异常)。胸痛的3个主要原因是肌肉骨骼问题(33%)、特发性(24.4%)和心因性(21.6%),心脏病因占1.1%。不到3%的患者需要住院,18.9%的患者被安排门诊咨询。有7.1%的再入院报告。与其他病因组相比,心因性胸痛在女性、青少年、有精神病史、既往有应激事件以及体格检查正常方面存在统计学上的显著关联。其中,不到30%的患者被安排到儿童精神病学/心理学咨询。
与分诊时的低优先级、诊断为良性以及低住院率相反,进行了大量补充诊断检查,但结果异常的很少。心因性胸痛出院后转诊率较低。作者强调临床算法对于减少不必要检查和再入院以及改善转诊和随访的重要性,特别是在心因性病因方面。