Chong Shu-Ling, Goh Mark Sen Liang, Ong Gene Yong-Kwang, Acworth Jason, Sultana Rehena, Yao Sarah Hui Wen, Ng Kee Chong
Department of Emergency Medicine, KK Women's and Children's Hospital, Singapore 100, Bukit Timah Road, Singapore 229899, Singapore.
Duke-NUS Medical School, Singapore 8 College Road, Singapore 169857, Singapore.
Resusc Plus. 2022 Jun 29;11:100262. doi: 10.1016/j.resplu.2022.100262. eCollection 2022 Sep.
We conducted a systematic review and meta-analysis to answer the question: Does the implementation of Paediatric Early Warning Systems (PEWS) in the hospital setting reduce mortality, cardiopulmonary arrests, unplanned codes and critical deterioration events among children, as compared to usual care without PEWS?
We conducted a comprehensive search using Medline, EMBASE, Cochrane Central Register of Controlled Trials, Cumulative Index to Nursing and Allied Health Literature and Web of Science. We included studies published between January 2006 and April 2022 on children <18 years old performed in inpatient units and emergency departments, and compared patient populations with PEWS to those without PEWS. We excluded studies without a comparator, case control studies, systematic reviews, and studies published in non-English languages. We employed a random effects meta-analysis and synthesised the risk and rate ratios from individual studies. We used the Scottish Intercollegiate Guidelines Network (SIGN) to appraise the risk of bias.
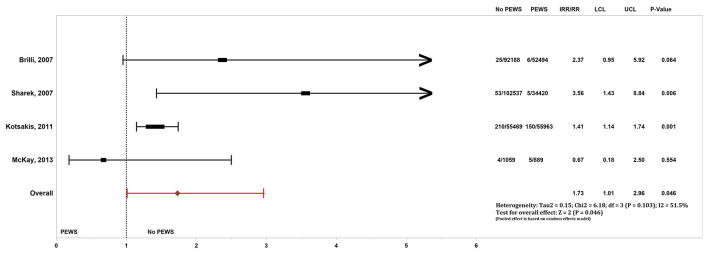
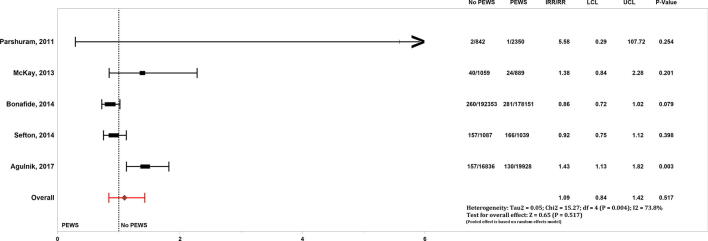
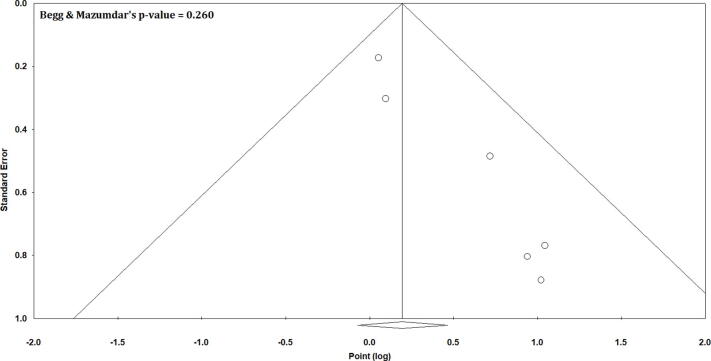
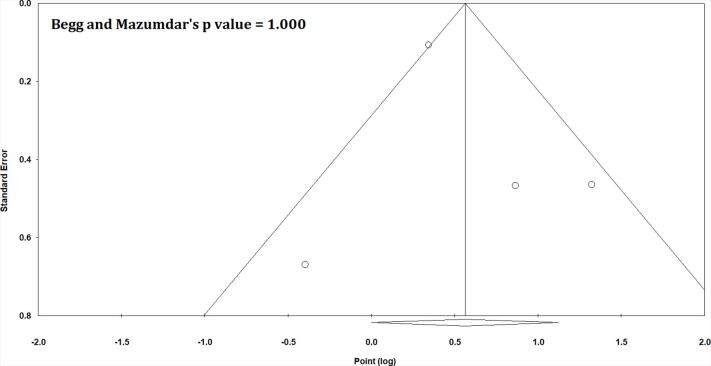
Among 911 articles screened, 15 were included for descriptive analysis. Fourteen of the 15 studies were pre- versus post-implementation studies and one was a multi-centre cluster randomised controlled trial (RCT). Among 10 studies (580,604 hospital admissions) analysed for mortality, we found an increased risk (pooled RR 1.18, 95% CI 1.01-1.38, = 0.036) in the group without PEWS compared to the group with PEWS. The sensitivity analysis performed without the RCT (436,065 hospital admissions) showed a non-significant relationship (pooled RR 1.17, 95% CI 0.98-1.40, = 0.087). Among four studies (168,544 hospital admissions) analysed for unplanned code events, there was an increased risk in the group without PEWS (pooled RR 1.73, 95%CI 1.01-2.96, = 0.046) There were no differences in the rate of cardiopulmonary arrests or critical deterioration events between groups. Our findings were limited by potential confounders and imprecision among included studies.
Healthcare systems that implemented PEWS were associated with reduced mortality and code rates. We recognise that these gains vary depending on resource availability and efferent response systems.PROSPERO registration: CRD42021269579.
我们进行了一项系统评价和荟萃分析,以回答以下问题:与未实施儿科早期预警系统(PEWS)的常规护理相比,在医院环境中实施PEWS是否能降低儿童的死亡率、心肺骤停、非计划抢救和病情严重恶化事件的发生率?
我们使用Medline、EMBASE、Cochrane对照试验中央注册库、护理及相关健康文献累积索引和科学网进行了全面检索。我们纳入了2006年1月至2022年4月期间发表的、在住院病房和急诊科对18岁以下儿童进行的研究,并将实施PEWS的患者群体与未实施PEWS的患者群体进行比较。我们排除了没有对照的研究、病例对照研究、系统评价以及非英文发表的研究。我们采用随机效应荟萃分析,并综合了各个研究的风险比和率比。我们使用苏格兰校际指南网络(SIGN)来评估偏倚风险。
在筛选的911篇文章中,有15篇被纳入进行描述性分析。15项研究中的14项是实施前与实施后的研究,1项是多中心整群随机对照试验(RCT)。在分析死亡率的10项研究(580,604例住院患者)中,我们发现与实施PEWS的组相比,未实施PEWS的组风险增加(合并RR 1.18,95%CI 1.01-1.38,P = 0.036)。在不包括RCT的情况下进行的敏感性分析(436,065例住院患者)显示无显著相关性(合并RR 1.17,95%CI 0.98-1.40,P = 0.087)。在分析非计划抢救事件的4项研究(168,544例住院患者)中,未实施PEWS的组风险增加(合并RR 1.73,95%CI 1.01-2.96,P = 0.046)。两组之间的心肺骤停率或病情严重恶化事件发生率没有差异。我们的研究结果受到纳入研究中潜在混杂因素和不精确性的限制。
实施PEWS的医疗保健系统与降低死亡率和抢救率相关。我们认识到这些益处因资源可用性和应急反应系统而异。PROSPERO注册号:CRD42021269579。