Buckley Benjamin J R, Lane Deirdre A, Calvert Peter, Zhang Juqian, Gent David, Mullins C Daniel, Dorian Paul, Kohsaka Shun, Hohnloser Stefan H, Lip Gregory Y H
Liverpool Centre for Cardiovascular Science, University of Liverpool and Liverpool Heart & Chest Hospital, Liverpool L14 3PE, UK.
Cardiovascular and Metabolic Medicine, Institute of Life Course and Medical Sciences, Faculty of Health and Life Sciences, University of Liverpool, Liverpool L69 3BX, UK.
J Clin Med. 2022 Jun 30;11(13):3788. doi: 10.3390/jcm11133788.
There is a plethora of real-world data on the safety and effectiveness of direct-acting oral anticoagulants (DOACs); however, study heterogeneity has contributed to inconsistent findings. We compared the effectiveness and safety of apixaban with those of other direct-acting oral anticoagulants (DOACs) and vitamin K antagonists (VKA e.g., warfarin).
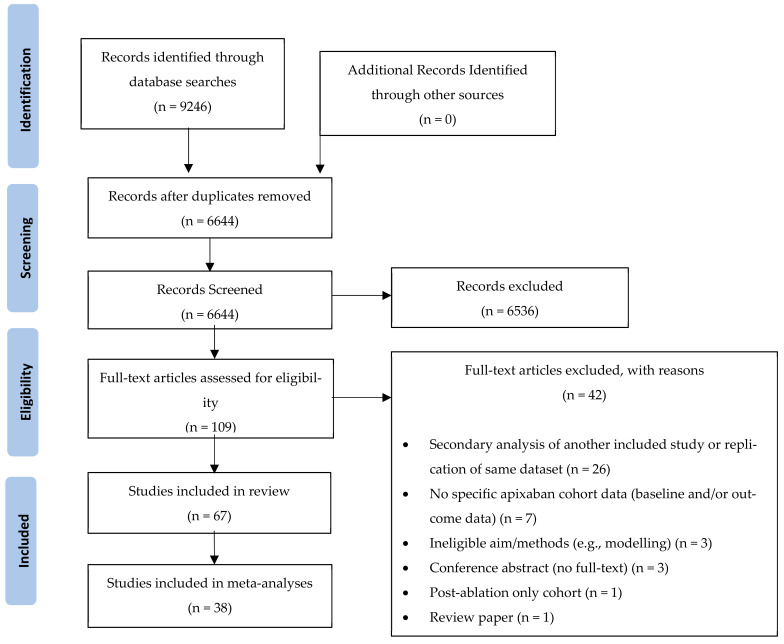
A systematic review and meta-analysis was conducted retrieving data from PubMed, SCOPUS and Web of Science from January 2009 to December 2021. Studies that evaluated apixaban (intervention) prescribed for adults (aged 18 years or older) with AF for stroke prevention compared to other DOACs or VKAs were identified. Primary outcomes included stroke/systemic embolism (SE), all-cause mortality, and major bleeding. Secondary outcomes were intracranial haemorrhage (ICH) and ischaemic stroke. Randomised controlled trials and non-randomised trials were considered for inclusion.
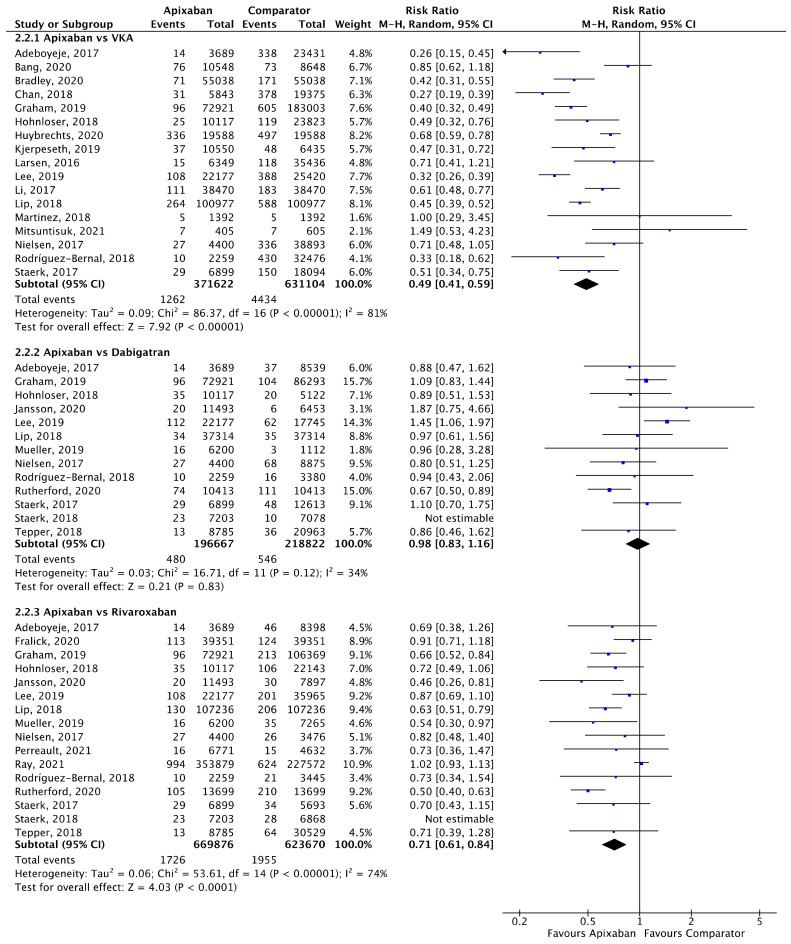
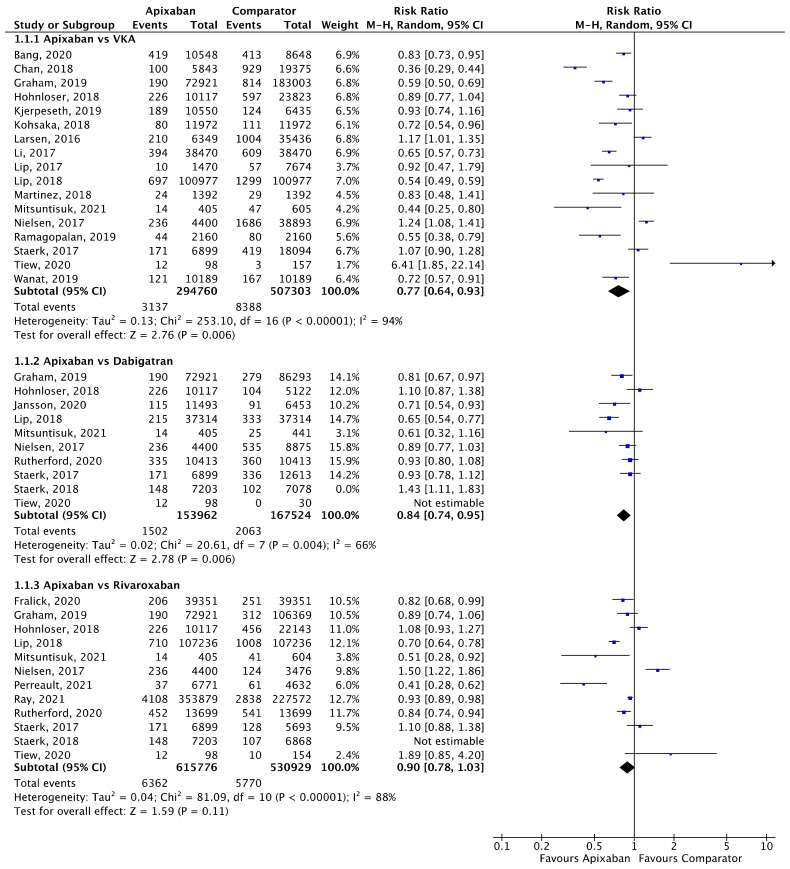
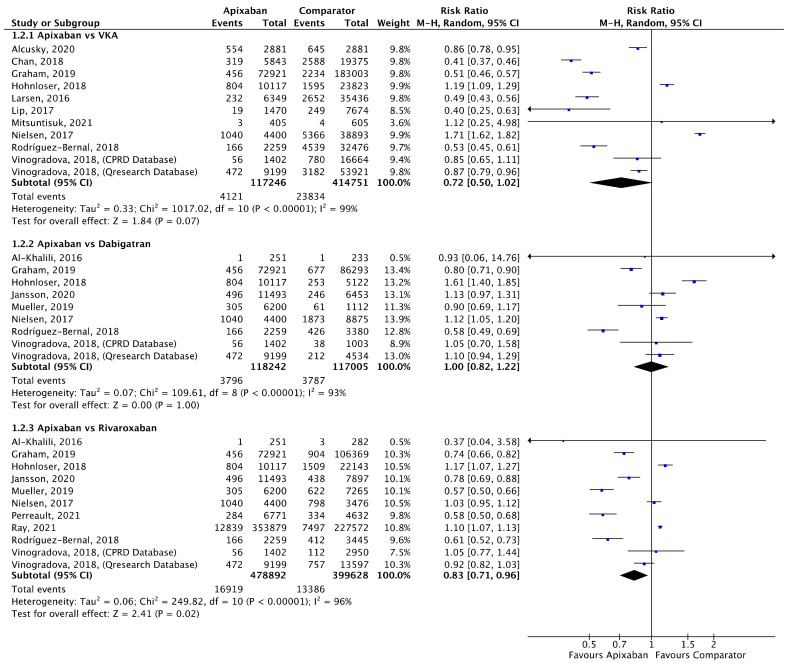
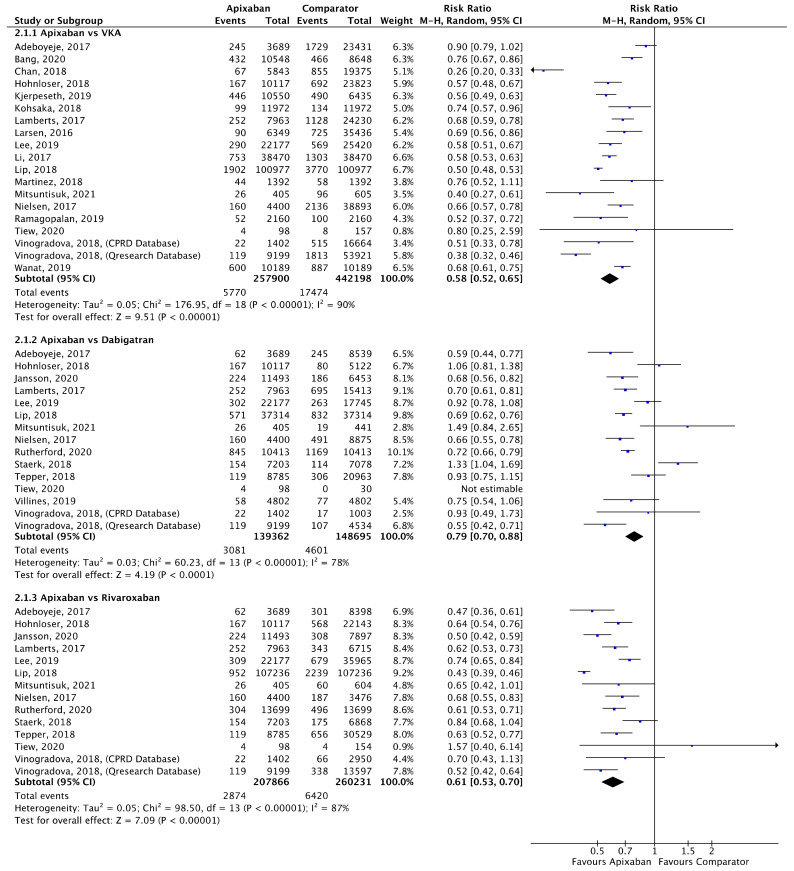
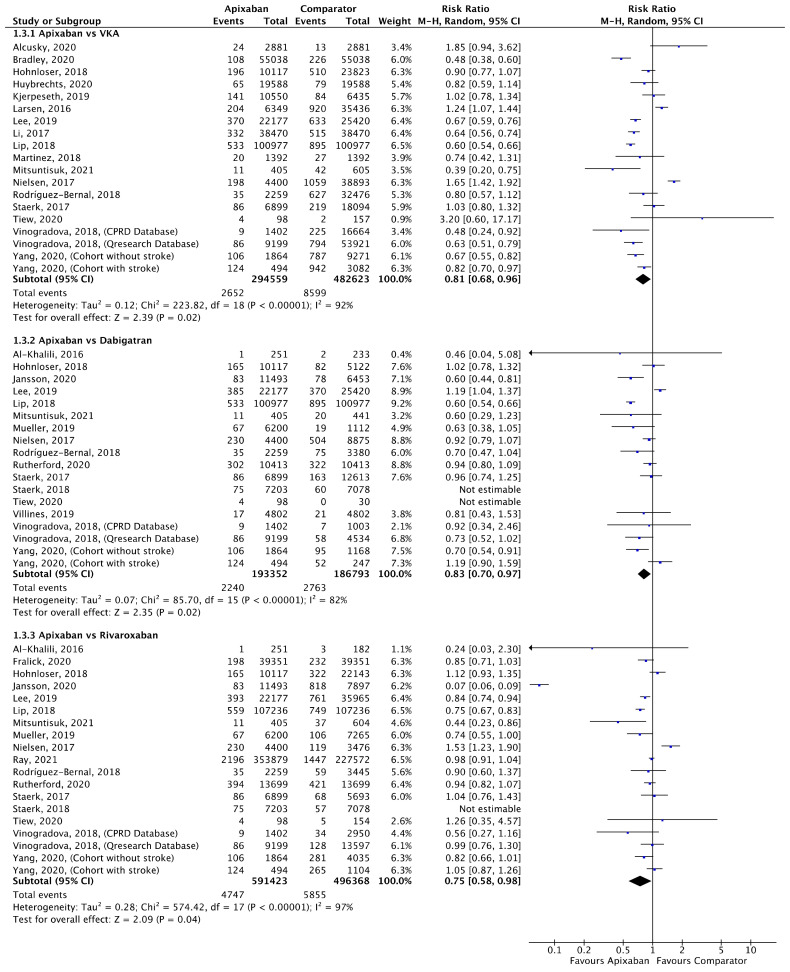
In total, 67 studies were included, and 38 studies were meta-analysed. Participants taking apixaban had significantly lower stroke/SE compared to patients taking VKAs (relative risk (RR) 0.77, 95% confidence interval (CI) 0.64-0.93, I = 94%) and dabigatran (RR 0.84, 95% CI 0.74-0.95, I = 66%), but not to patients administered rivaroxaban. There was no statistical difference in mortality between apixaban and VKAs or apixaban and dabigatran. Compared to patients administered rivaroxaban, participants taking apixaban had lower mortality rates (RR 0.83, 95% CI 0.71-0.96, I = 96%). Apixaban was associated with a significantly lower risk of major bleeding compared to VKAs (RR 0.58, 95% CI 0.52-0.65, I = 90%), dabigatran (RR 0.79, 95% CI 0.70-0.88, I = 78%) and rivaroxaban (RR 0.61, 95% CI 0.53-0.70, I = 87%).
Apixaban was associated with a better overall safety and effectiveness profile compared to VKAs and other DOACs.
关于直接口服抗凝剂(DOACs)的安全性和有效性,有大量的真实世界数据;然而,研究的异质性导致了结果不一致。我们比较了阿哌沙班与其他直接口服抗凝剂(DOACs)以及维生素K拮抗剂(VKA,如华法林)的有效性和安全性。
进行了一项系统评价和荟萃分析,检索了2009年1月至2021年12月期间来自PubMed、SCOPUS和Web of Science的数据。确定了评估为预防中风而给成年(18岁及以上)房颤患者开具阿哌沙班(干预措施)与其他DOACs或VKAs进行比较的研究。主要结局包括中风/全身性栓塞(SE)、全因死亡率和大出血。次要结局为颅内出血(ICH)和缺血性中风。纳入随机对照试验和非随机试验。
总共纳入67项研究,其中38项研究进行了荟萃分析。与服用VKA的患者相比,服用阿哌沙班的参与者中风/SE显著更低(相对风险(RR)0.77,95%置信区间(CI)0.64 - 0.93,I² = 94%)以及与达比加群相比(RR 0.84,95% CI 0.74 - 0.95,I² = 66%),但与服用利伐沙班的患者相比无差异。阿哌沙班与VKA之间或阿哌沙班与达比加群之间在死亡率上无统计学差异。与服用利伐沙班的患者相比,服用阿哌沙班的参与者死亡率更低(RR 0.83,95% CI 0.71 - 0.96,I² = 96%)。与VKA(RR 0.58,95% CI 0.52 - 0.65,I² = 90%)、达比加群(RR 0.79,95% CI 0.70 - 0.88,I² = 78%)和利伐沙班(RR 0.61,95% CI 0.53 - 0.70,I² = 87%)相比,阿哌沙班大出血风险显著更低。
与VKA和其他DOACs相比,阿哌沙班具有更好的总体安全性和有效性。