Australian Cancer Research Foundation, Department of Cancer Biology and Therapeutics, John Curtin School of Medical Research, The Australian National University, Canberra, Australian Capital Territory, Australia.
Department of Haematology, Canberra Hospital, Canberra, Australian Capital Territory, Australia.
Thromb Haemost. 2022 Nov;122(11):1843-1857. doi: 10.1055/a-1896-7092. Epub 2022 Jul 11.
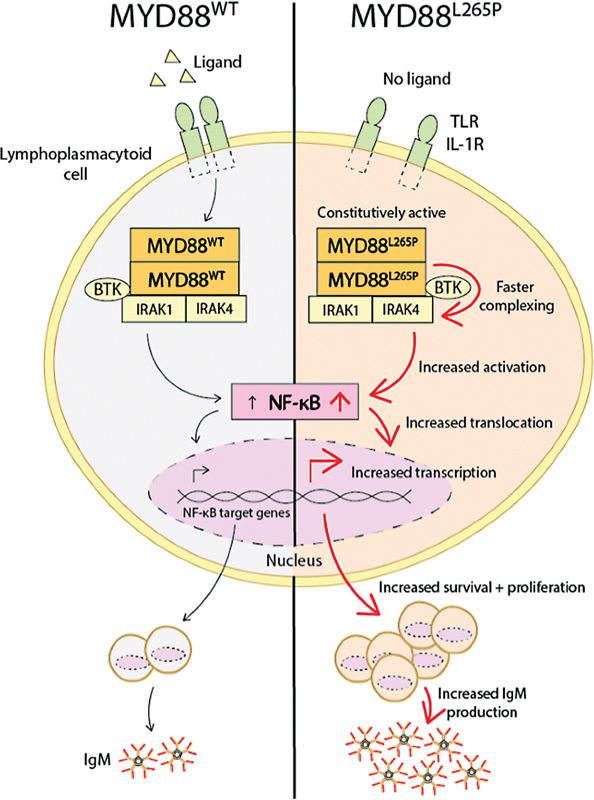
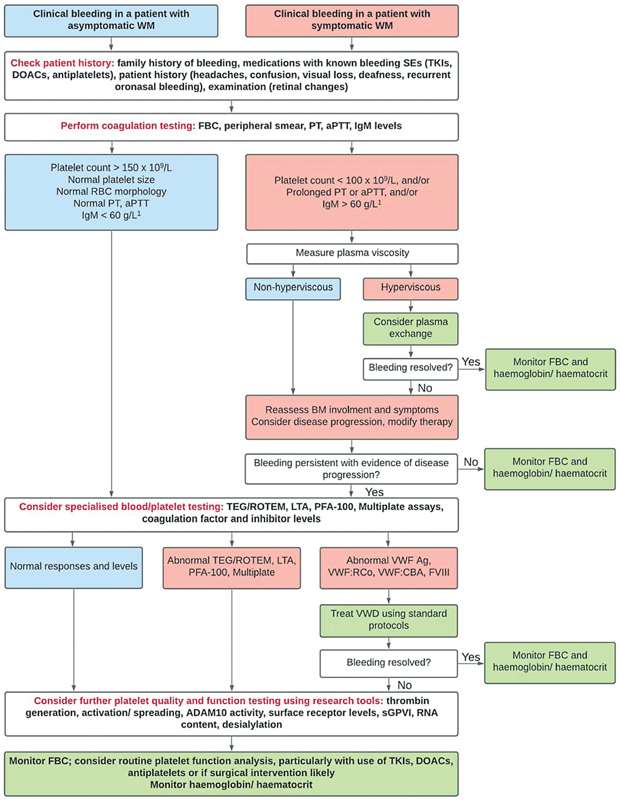
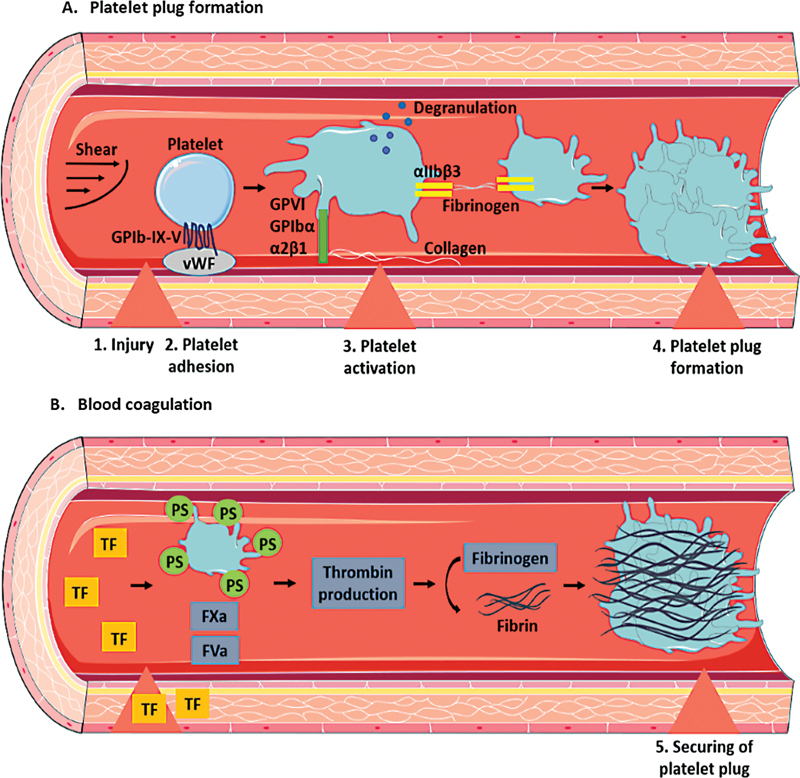
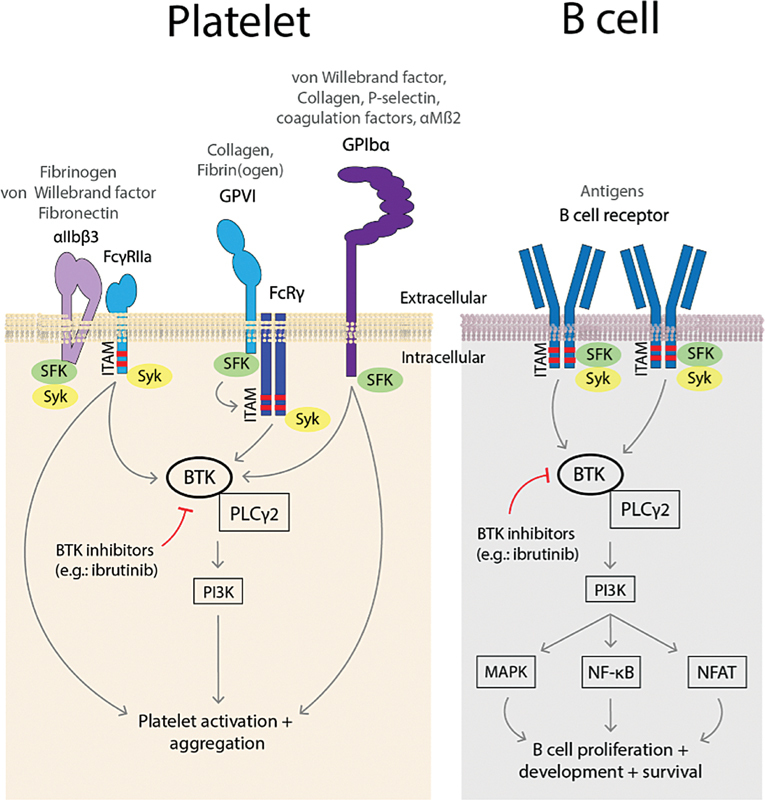
Waldenström macroglobulinemia (WM) is a rare, incurable, low-grade, B cell lymphoma. Symptomatic disease commonly results from marrow or organ infiltration and hyperviscosity secondary to immunoglobulin M paraprotein, manifesting as anemia, bleeding and neurological symptoms among others. The causes of the bleeding phenotype in WM are complex and involve several intersecting mechanisms. Evidence of defects in platelet function is lacking in the literature, but factors impacting platelet function and coagulation pathways such as acquired von Willebrand factor syndrome, hyperviscosity, abnormal hematopoiesis, cryoglobulinemia and amyloidosis may contribute to bleeding. Understanding the pathophysiological mechanisms behind bleeding is important, as common WM therapies, including chemo-immunotherapy and Bruton's tyrosine kinase inhibitors, carry attendant bleeding risks. Furthermore, due to the relatively indolent nature of this lymphoma, most patients diagnosed with WM are often older and have one or more comorbidities, requiring treatment with anticoagulant or antiplatelet drugs. It is thus important to understand the origin of the WM bleeding phenotype, to better stratify patients according to their bleeding risk, and enhance confidence in clinical decisions regarding treatment management. In this review, we detail the evidence for various contributing factors to the bleeding phenotype in WM and focus on current and emerging diagnostic tools that will aid evaluation and management of bleeding in these patients.
华氏巨球蛋白血症(WM)是一种罕见的、无法治愈的、低级别的 B 细胞淋巴瘤。症状性疾病通常是由于骨髓或器官浸润以及免疫球蛋白 M 副蛋白引起的高粘滞血症引起的,表现为贫血、出血和神经症状等。WM 出血表型的原因较为复杂,涉及多种相互交叉的机制。文献中缺乏血小板功能缺陷的证据,但影响血小板功能和凝血途径的因素,如获得性血管性血友病综合征、高粘滞血症、异常造血、冷球蛋白血症和淀粉样变性,可能导致出血。了解出血背后的病理生理机制非常重要,因为常见的 WM 治疗方法,包括化疗免疫治疗和布鲁顿酪氨酸激酶抑制剂,都伴有出血风险。此外,由于这种淋巴瘤的性质相对惰性,大多数诊断为 WM 的患者通常年龄较大,并有一个或多个合并症,需要使用抗凝或抗血小板药物进行治疗。因此,了解 WM 出血表型的起源,根据出血风险对患者进行分层,并增强对治疗管理相关临床决策的信心非常重要。在本综述中,我们详细介绍了导致 WM 出血表型的各种因素的证据,并重点介绍了当前和新兴的诊断工具,这些工具将有助于评估和管理这些患者的出血情况。