Chen Dong-Yi, Liu Jia-Rou, Tseng Chi-Nan, Hsieh Ming-Jer, Chuang Cheng-Keng, Pang See-Tong, Chen Shao-Wei, Hsieh I-Chang, Chu Pao-Hsien, Chen Jen-Shi, Wen-Cheng Chang John, Huang Wen-Kuan, See Lai-Chu
Division of Cardiology, Department of Internal Medicine, Chang Gung Memorial Hospital at Linkou, Chang Gung University College of Medicine, Taoyuan, Taiwan.
Department of Public Health, College of Medicine, Chang Gung University, Taoyuan, Taiwan.
JACC CardioOncol. 2022 Jun 21;4(2):223-234. doi: 10.1016/j.jaccao.2022.05.002. eCollection 2022 Jun.
The risk for major adverse cardiovascular events (MACE) with targeted therapies for patients with advanced renal cell carcinoma (RCC) in real-world practice remains unclear.
The aim of this study was to compare the risk for MACE associated with targeted cancer therapies with that associated with cytokine treatment in patients with advanced RCC.
Using Taiwan's National Health Insurance Research Database, a retrospective nationwide cohort study was conducted involving patients with advanced RCC who had received targeted therapy (sunitinib, sorafenib, pazopanib, everolimus, or temsirolimus) or cytokine therapy (interleukin-2 or interferon gamma) from 2007 to 2018. Cox proportional hazards models were used to estimate the risk for MACE (a composite of myocardial infarction, ischemic stroke, heart failure, and cardiovascular death) in the cohort using the propensity score method of stabilized inverse probability of treatment weighting.
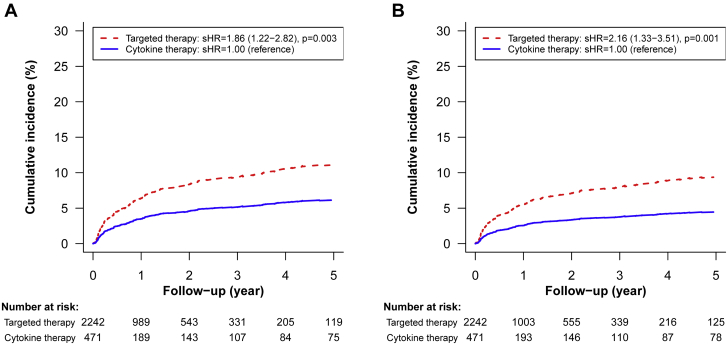
In this cohort of 2,785 patients with advanced RCC, 2,257 (81%) and 528 (19%) had received targeted and cytokine therapy, respectively. After stabilized inverse probability of treatment weighting, the incidence rates of MACE were 6.65 and 3.36 per 100 person-years in the targeted and cytokine therapy groups, respectively (HR: 1.80; 95% CI: 1.19-2.74). Baseline history of heart failure (HR: 3.88; 95% CI: 2.25-6.71), atrial fibrillation (HR: 3.60; 95% CI: 2.16-5.99), venous thromboembolism (HR: 2.50; 95% CI: 1.27-4.92), ischemic stroke (HR: 1.88; 95% CI: 1.14-3.11), and age ≥ 65 years (HR: 1.81; 95% CI: 1.27-2.58) were independent risk factors for targeted therapy-associated MACE.
Among patients with advanced RCC, the risk for MACE associated with targeted cancer therapy is higher than that associated with cytokine therapy.
在实际临床实践中,晚期肾细胞癌(RCC)患者接受靶向治疗后发生主要不良心血管事件(MACE)的风险仍不明确。
本研究旨在比较晚期RCC患者接受靶向抗癌治疗与细胞因子治疗后发生MACE的风险。
利用台湾地区国民健康保险研究数据库,开展一项全国性回顾性队列研究,纳入2007年至2018年期间接受靶向治疗(舒尼替尼、索拉非尼、帕唑帕尼、依维莫司或替西罗莫司)或细胞因子治疗(白细胞介素-2或干扰素γ)的晚期RCC患者。采用Cox比例风险模型,运用倾向评分法进行稳定逆概率处理加权,评估队列中发生MACE(心肌梗死、缺血性卒中、心力衰竭和心血管死亡的复合事件)的风险。
在这一包含2785例晚期RCC患者的队列中,分别有2257例(81%)和528例(19%)接受了靶向治疗和细胞因子治疗。经过稳定逆概率处理加权后,靶向治疗组和细胞因子治疗组的MACE发病率分别为每100人年6.65例和3.36例(风险比:1.80;95%置信区间:1.19 - 2.74)。心力衰竭基线病史(风险比:3.88;95%置信区间:2.25 - 6.71)、心房颤动(风险比:3.60;95%置信区间:2.16 - 5.99)、静脉血栓栓塞(风险比:2.50;95%置信区间:1.27 - 4.92)、缺血性卒中(风险比:1.88;95%置信区间:1.14 - 3.11)以及年龄≥65岁(风险比:1.81;95%置信区间:1.27 - 2.58)是靶向治疗相关MACE的独立危险因素。
在晚期RCC患者中,靶向抗癌治疗相关的MACE风险高于细胞因子治疗。