Defence Science and Technology Laboratory, Porton Down, Salisbury, Wiltshire, UK.
Bloomsbury Institute of Intensive Care Medicine, Division of Medicine, University College London, London, UK.
Intensive Care Med. 2022 Sep;48(9):1133-1143. doi: 10.1007/s00134-022-06769-z. Epub 2022 Jul 13.
Early accurate diagnosis of infection ± organ dysfunction (sepsis) remains a major challenge in clinical practice. Utilizing effective biomarkers to identify infection and impending organ dysfunction before the onset of clinical signs and symptoms would enable earlier investigation and intervention. To our knowledge, no prior study has specifically examined the possibility of pre-symptomatic detection of sepsis.
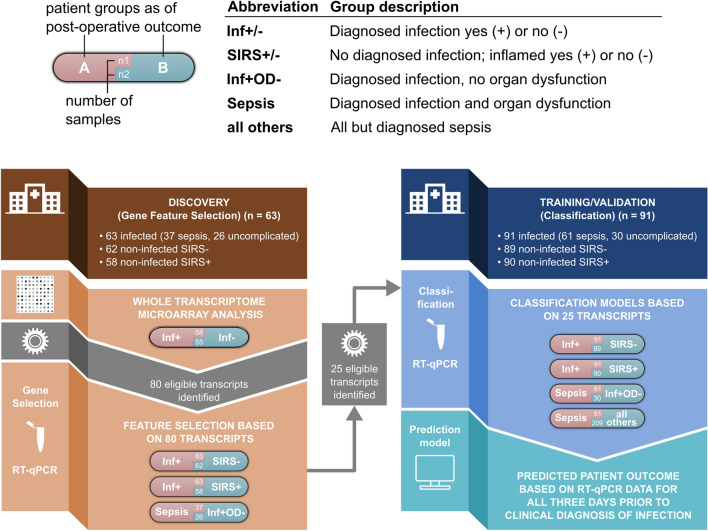
Blood samples and clinical/laboratory data were collected daily from 4385 patients undergoing elective surgery. An adjudication panel identified 154 patients with definite postoperative infection, of whom 98 developed sepsis. Transcriptomic profiling and subsequent RT-qPCR were undertaken on sequential blood samples taken postoperatively from these patients in the three days prior to the onset of symptoms. Comparison was made against postoperative day-, age-, sex- and procedure- matched patients who had an uncomplicated recovery (n =151) or postoperative inflammation without infection (n =148).
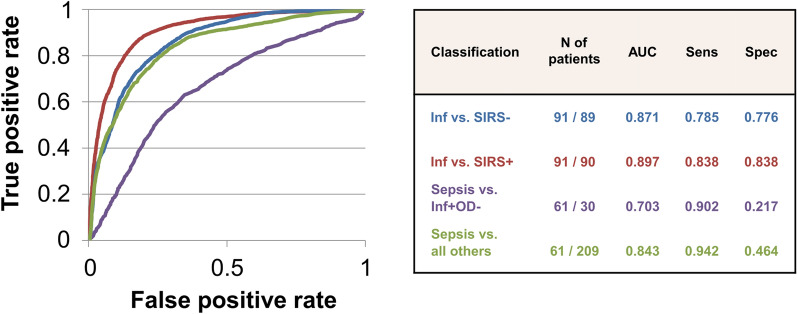
Specific gene signatures optimized to predict infection or sepsis in the three days prior to clinical presentation were identified in initial discovery cohorts. Subsequent classification using machine learning with cross-validation with separate patient cohorts and their matched controls gave high Area Under the Receiver Operator Curve (AUC) values. These allowed discrimination of infection from uncomplicated recovery (AUC 0.871), infectious from non-infectious systemic inflammation (0.897), sepsis from other postoperative presentations (0.843), and sepsis from uncomplicated infection (0.703).
Host biomarker signatures may be able to identify postoperative infection or sepsis up to three days in advance of clinical recognition. If validated in future studies, these signatures offer potential diagnostic utility for postoperative management of deteriorating or high-risk surgical patients and, potentially, other patient populations.
早期准确诊断感染±器官功能障碍(脓毒症)仍然是临床实践中的主要挑战。利用有效的生物标志物在出现临床症状和体征之前识别感染和即将发生的器官功能障碍,将能够更早地进行检查和干预。据我们所知,以前没有研究专门探讨过在症状出现前检测脓毒症的可能性。
从 4385 名接受择期手术的患者中每天采集血液样本和临床/实验室数据。一个裁决小组确定了 154 名术后明确感染的患者,其中 98 名患者发生了脓毒症。对这些患者在出现症状前三天内术后采集的连续血样进行转录组谱分析和随后的 RT-qPCR。与术后无并发症恢复的患者(n=151)或术后无感染的炎症患者(n=148)进行比较,这些患者在年龄、性别和手术程序上相匹配。
在最初的发现队列中,针对症状出现前三天预测感染或脓毒症的特定基因特征进行了优化。使用机器学习进行后续分类,并使用来自不同患者队列及其匹配对照的交叉验证进行分类,获得了较高的接收器操作特征曲线(AUC)值。这些方法可以区分感染与无并发症的恢复(AUC 0.871)、感染与非感染性全身炎症(0.897)、脓毒症与其他术后表现(0.843)、以及脓毒症与无并发症的感染(0.703)。
宿主生物标志物特征可能能够在临床识别之前提前三天识别术后感染或脓毒症。如果在未来的研究中得到验证,这些特征为恶化或高危手术患者的术后管理以及潜在的其他患者群体提供了潜在的诊断效用。