Yu Priscilla, Esangbedo Ivie, Li Xilong, Wolovits Joshua, Thiagarajan Ravi, Raman Lakshmi
Division of Critical Care, Department of Pediatrics, University of Texas Southwestern Medical Center, Dallas, TX, United States.
Division of Cardiac Critical Care, Department of Pediatrics, University of Washington Seattle, Seattle, WA, United States.
Front Pediatr. 2022 Jun 27;10:894125. doi: 10.3389/fped.2022.894125. eCollection 2022.
The association of near-infrared spectroscopy (NIRS) with various outcomes after pediatric cardiac surgery has been studied extensively. However, the role of NIRS in the prediction of cardiac arrest (CA) in children with heart disease has yet to be evaluated. We sought to determine if a model utilizing regional cerebral oximetry (rSO2c) and somatic oximetry (rSO2s) could predict CA in children admitted to a single-center pediatric cardiac intensive care unit (CICU).
We retrospectively reviewed 160 index CA events for patients admitted to our pediatric CICU between November 2010 and January 2019. We selected 711 control patients who did not have a cardiac arrest. Hourly data was collected from the electronic health record (EHR). We previously created a machine-learning algorithm to predict the risk of CA using EHR data. Univariable analysis was done on these variables, which we then used to create a multivariable logistic regression model. The outputs from the model were presented by odds ratio (OR) and 95% confidence interval (CI).
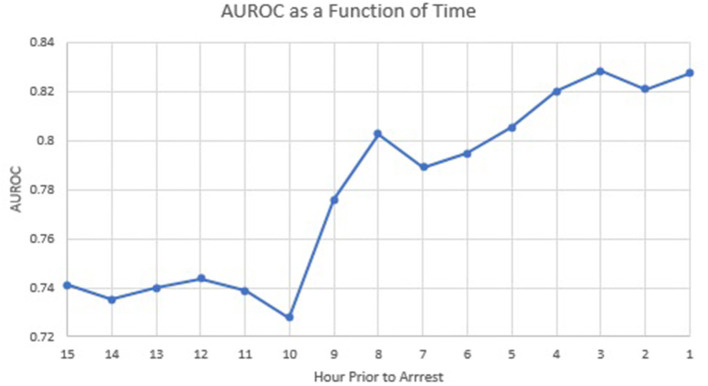
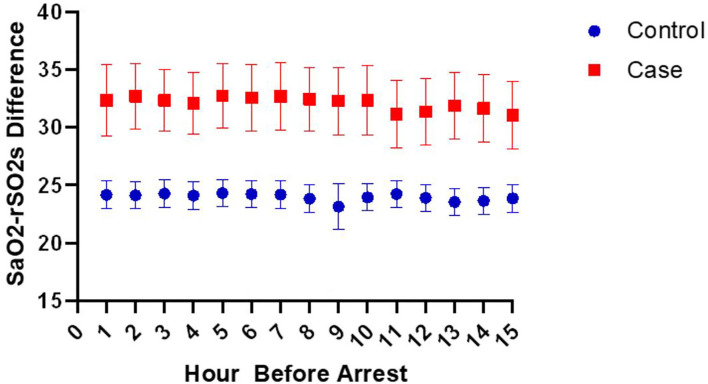
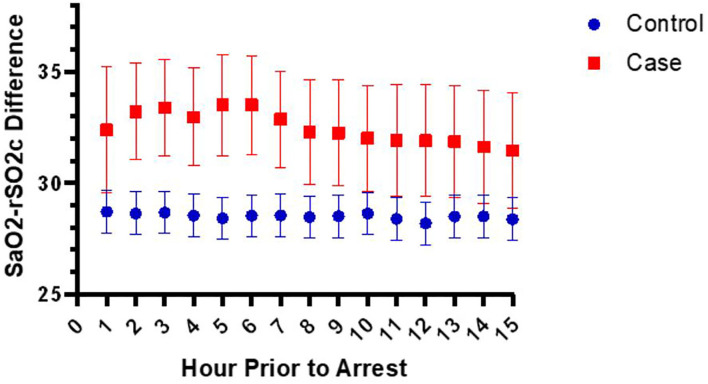
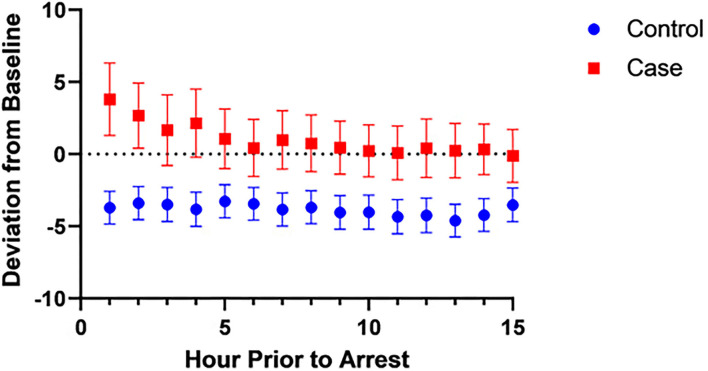
We created a multivariable model to evaluate the association of CA using five variables: arterial saturation (SpO2)- rSO2c difference, SpO2-rSO2s difference, heart rate, diastolic blood pressure, and vasoactive inotrope score. While the SpO2-rSO2c difference was not a significant contributor to the multivariable model, the SpO2-rSO2s difference was. The average SpO2-rSO2s difference cutoff with the best prognostic accuracy for CA was 29% [CI 26-31%]. In the multivariable model, a 10% increase in the SpO2-rSO2s difference was independently associated with increased odds of CA [OR 1.40 (1.18, 1.67), < 0.001] at 1 h before CA. Our model predicted CA with an AUROC of 0.83 at 1 h before CA.
In this single-center case-control study of children admitted to a pediatric CICU, we created a multivariable model utilizing hourly data from the EHR to predict CA. At 1 h before the event, for every 10% increase in the SpO2-rSO2s difference, the odds of cardiac arrest increased by 40%. These findings are important as the field explores ways to capitalize on the wealth of data at our disposal to improve patient care.
近红外光谱(NIRS)与小儿心脏手术后各种结局的关联已得到广泛研究。然而,NIRS在预测患有心脏病的儿童心脏骤停(CA)方面的作用尚未得到评估。我们试图确定一个利用局部脑血氧饱和度(rSO2c)和体部血氧饱和度(rSO2s)的模型是否能够预测入住单中心小儿心脏重症监护病房(CICU)的儿童发生CA的情况。
我们回顾性分析了2010年11月至2019年1月期间入住我院小儿CICU的患者发生的160例首次CA事件。我们选取了711例未发生心脏骤停的对照患者。每小时的数据从电子健康记录(EHR)中收集。我们之前创建了一种机器学习算法,使用EHR数据预测CA风险。对这些变量进行单变量分析,然后用于创建多变量逻辑回归模型。模型的输出以比值比(OR)和95%置信区间(CI)表示。
我们创建了一个多变量模型,使用五个变量评估CA的关联:动脉血氧饱和度(SpO2)-rSO2c差值、SpO2-rSO2s差值、心率、舒张压和血管活性正性肌力评分。虽然SpO2-rSO2c差值对多变量模型的贡献不显著,但SpO2-rSO2s差值是显著的。预测CA的最佳预后准确性的平均SpO2-rSO2s差值临界值为29%[CI 26-31%]。在多变量模型中,CA前1小时SpO2-rSO2s差值每增加10%与CA发生几率增加独立相关[OR 1.40(1.18,1.67),<0.001]。我们的模型在CA前1小时预测CA的曲线下面积(AUROC)为0.83。
在这项针对入住小儿CICU的儿童的单中心病例对照研究中,我们创建了一个利用EHR每小时数据预测CA的多变量模型。在事件发生前1小时,SpO2-rSO2s差值每增加10%,心脏骤停的几率增加40%。随着该领域探索如何利用我们可获得的大量数据来改善患者护理,这些发现具有重要意义。