Division of Hematology, Department of Internal Medicine, Faculty of Medicine, University of Debrecen, Debrecen, Hungary.
Doctoral School of Clinical Medicine, University of Debrecen, Debrecen, Hungary.
Ann Hematol. 2022 Oct;101(10):2337-2345. doi: 10.1007/s00277-022-04924-6. Epub 2022 Jul 14.
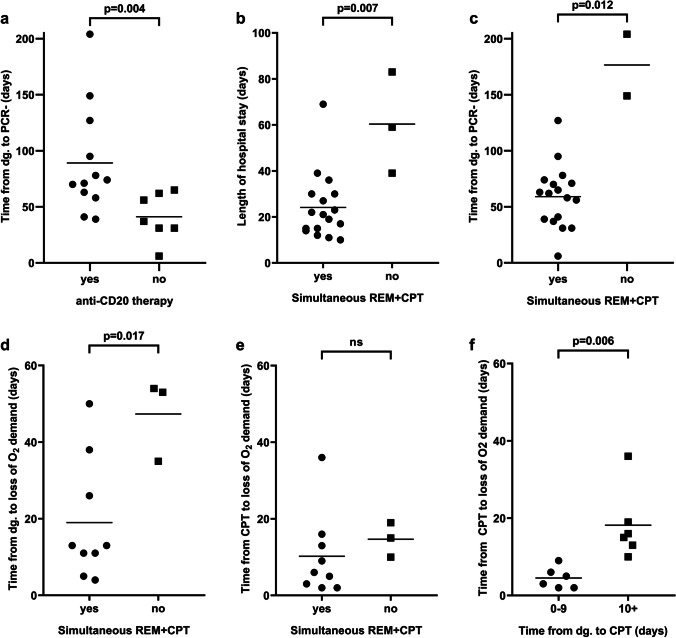
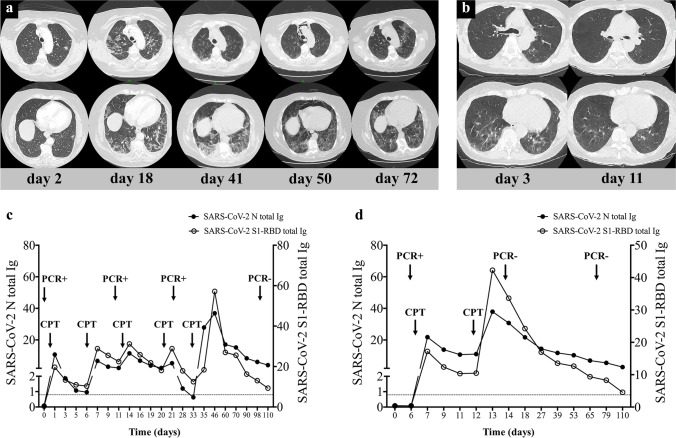
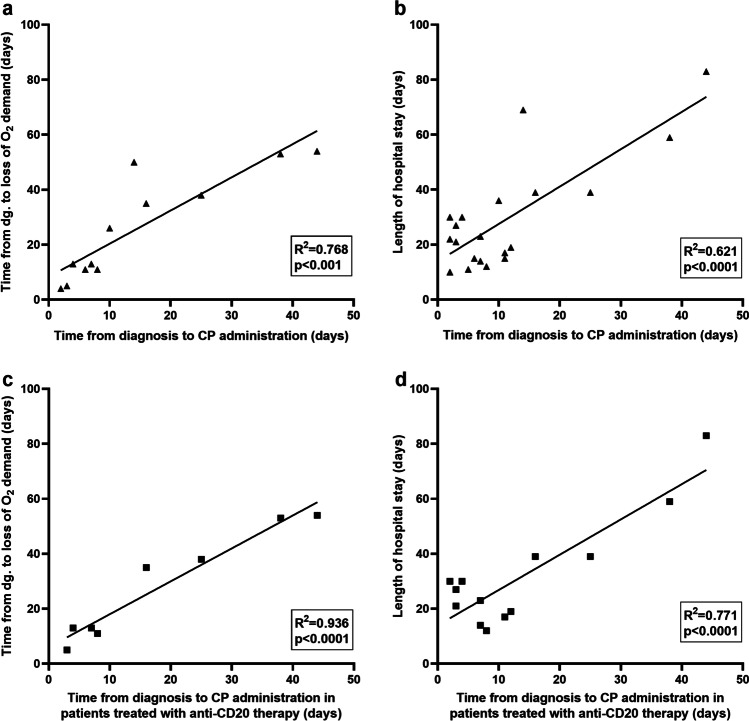
Patients with hematological malignancies (HMs) are at a higher risk of developing severe form and protracted course of COVID-19 disease. We investigated whether the combination of viral replication inhibition with remdesivir and administration of anti-SARS-CoV-2 immunoglobulins with convalescent plasma (CP) therapy might be sufficient to treat B-cell-depleted patients with COVID-19. We enrolled 20 consecutive patients with various HMs with profound B-cell lymphopenia and COVID-19 pneumonia between December 2020 and May 2021. All patients demonstrated undetectable baseline anti-SARS-CoV-2 immunoglobulin levels before CP. Each patient received at least a complete course of remdesivir and at least one unit of CP. Previous anti-CD20 therapy resulted in a more prolonged SARS-CoV-2 PCR positivity compared to other causes of B-cell lymphopenia (p = 0.004). Timing of CP therapy showed a significant impact on the clinical outcome. Simultaneous use of remdesivir and CP reduced time period for oxygen weaning after diagnosis (p = 0.017), length of hospital stay (p = 0.007), and PCR positivity (p = 0.012) compared to patients who received remdesivir and CP consecutively. In addition, time from the diagnosis to CP therapy affected the length of oxygen dependency (p < 0.001) and hospital stay (p < 0.0001). In those cases where there were at least 10 days from the diagnosis to plasma administration, oxygen dependency was prolonged vs. patients with shorter interval (p = 0.006). In conclusion, the combination of inhibition of viral replication with passive immunization was proved to be efficient and safe. Our results suggest the clear benefit of early, combined administration of remdesivir and CP to avoid protracted COVID-19 disease among patients with HMs and B-cell lymphopenia.
患有血液恶性肿瘤(HM)的患者发生 COVID-19 重症和病程延长的风险较高。我们研究了病毒复制抑制联合瑞德西韦和抗 SARS-CoV-2 免疫球蛋白与恢复期血浆(CP)治疗相结合是否足以治疗 COVID-19 耗竭 B 细胞的患者。我们纳入了 20 例 2020 年 12 月至 2021 年 5 月期间患有各种 HM 并伴有严重 B 细胞淋巴细胞减少和 COVID-19 肺炎的连续患者。所有患者在接受 CP 治疗前的基线均检测不到抗 SARS-CoV-2 免疫球蛋白水平。每位患者至少接受了完整疗程的瑞德西韦和至少 1 个单位的 CP。与其他 B 细胞淋巴细胞减少症的原因相比,先前的抗 CD20 治疗导致 SARS-CoV-2 PCR 阳性持续时间更长(p=0.004)。CP 治疗的时机对临床结果有显著影响。瑞德西韦和 CP 同时使用可减少确诊后脱机时间(p=0.017)、住院时间(p=0.007)和 PCR 阳性(p=0.012),与连续接受瑞德西韦和 CP 的患者相比。此外,从确诊到 CP 治疗的时间影响了氧依赖时间(p<0.001)和住院时间(p<0.0001)。在从确诊到血浆输注至少间隔 10 天的情况下,与间隔时间较短的患者相比,氧依赖时间延长(p=0.006)。总之,病毒复制抑制与被动免疫联合治疗被证明是有效和安全的。我们的研究结果表明,对于 HM 和 B 细胞淋巴细胞减少的患者,早期联合使用瑞德西韦和 CP 可避免 COVID-19 病程延长,具有明确的益处。