Stumpfe M C, Horch R E, Arkudas A, Cai A, Müller-Seubert W, Hauck T, Ludolph I
Department of Plastic and Hand Surgery, Laboratory for Tissue Engineering and Regenerative Medicine, University Hospital Erlangen, Friedrich-Alexander University Erlangen-Nürnberg (FAU), Erlangen, Germany.
Front Surg. 2022 Jun 28;9:867487. doi: 10.3389/fsurg.2022.867487. eCollection 2022.
Hidradenitis suppurativa is manifested by painful abscesses and scarring of sweat glands. Axillary, inguinal and genital regions are mostly affected. Multiple options exist in the treatment of hidradenitis suppurativa. The aim of this retrospective, mono-center cohort study was to analyze the outcome of different treatment methods after radical excision of hidradenitis suppurativa.
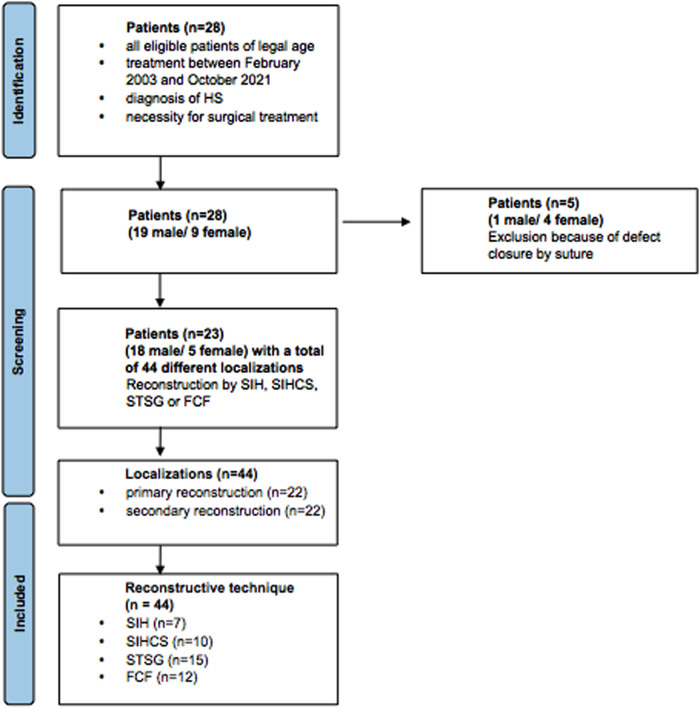
We retrospectively evaluated the treatment strategy and recurrence rate of hidradenitis suppurativa. We included all eligible patients of legal age between February 2003 and October 2021, with the diagnosis of Hidradenitis suppurativa and the necessity for surgical treatment. All patients with surgical treatment and direct wound closure by suture were excluded. Bacterial load and flora were analyzed for primary and secondary reconstruction in combination with negative-pressure wound therapy. Patient data were analyzed for recurrence rate and remission time according to different reconstructive techniques.
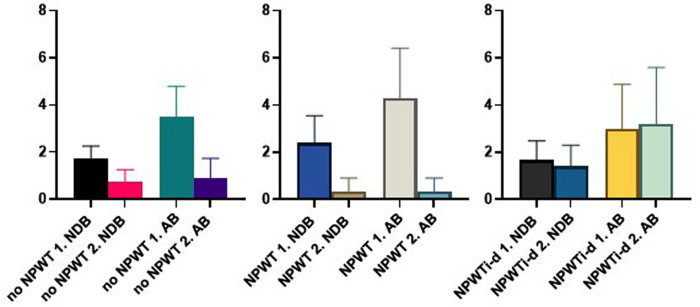
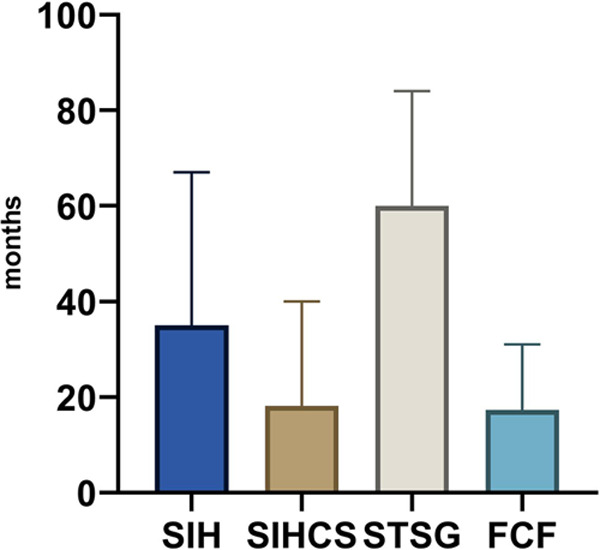
In 44 affected anatomical sites ( = 23 patients) we treated 15 patients with negative-pressure wound therapy. Bacterial load and flora were lower in the last wound swab of patients with multi-surgical procedures (22 localizations) compared to the first wound swab independent of the use of negative-pressure wound therapy.Wound closure, independent of a direct and multi-stage procedure was achieved by local fasciocutaneous flaps ( = 12), secondary intention healing ( = 7), secondary intention healing with buried chip skin grafts ( = 10), or splitthickness skin grafts ( = 15). Radical excision combined with splitthickness skin grafts showed the lowest recurrence rate in the follow-up (16%; = 4).
Radical excision of hidradenitis suppurativa as gold standard for surgical treatment combined with negative-pressure wound therapy as multi-stage procedures ultimately reduced bacterial load and flora in our study. The use of splitthickness skin grafts showed the lowest recurrence rate.
化脓性汗腺炎表现为疼痛性脓肿和汗腺瘢痕形成。腋窝、腹股沟和生殖器区域最常受累。化脓性汗腺炎的治疗有多种选择。这项回顾性单中心队列研究的目的是分析化脓性汗腺炎根治性切除术后不同治疗方法的效果。
我们回顾性评估了化脓性汗腺炎的治疗策略和复发率。纳入了2003年2月至2021年10月期间所有符合条件的法定年龄患者,这些患者被诊断为化脓性汗腺炎且有手术治疗的必要。所有接受手术治疗并通过缝合直接关闭伤口的患者均被排除。结合负压伤口治疗分析一期和二期重建的细菌载量和菌群。根据不同的重建技术分析患者数据的复发率和缓解时间。
在44个受累解剖部位(共23例患者),我们对15例患者采用了负压伤口治疗。与首次伤口拭子相比,多次手术(22个部位)患者的最后一次伤口拭子中的细菌载量和菌群较低,无论是否使用负压伤口治疗。伤口闭合,无论采用直接还是多阶段手术,均通过局部筋膜皮瓣(12例)、二期愈合(7例)、带埋植芯片皮片的二期愈合(10例)或中厚皮片移植(15例)实现。在随访中,根治性切除联合中厚皮片移植的复发率最低(16%;共4例)。
在我们的研究中,化脓性汗腺炎的根治性切除作为手术治疗的金标准,联合负压伤口治疗作为多阶段手术最终降低了细菌载量和菌群。中厚皮片移植的复发率最低。