Yamada Takehiro, Ohtakara Kazuhiro, Kamomae Takeshi, Itoh Junji, Shimada Hideki, Ishihara Shunichi, Naganawa Shinji
Department of Radiology, Toyohashi Municipal Hospital, Toyohashi, JPN.
Department of Radiation Oncology, Kainan Hospital Aichi Prefectural Welfare Federation of Agricultural Cooperatives, Yatomi, JPN.
Cureus. 2022 Jun 13;14(6):e25888. doi: 10.7759/cureus.25888. eCollection 2022 Jun.
Several factors, including the surrounding brain volume receiving specific doses, have hitherto been reported to correlate with brain radionecrosis (BR) after single or fractionated stereotactic radiosurgery (sSRS or fSRS) for brain metastases (BMs); however, those, especially for fSRS, have not yet been fully elucidated. Furthermore, the clinical outcome data of patients with BM treated with SRS using Vero4DRT are extremely limited. Therefore, this study aimed to demonstrate the incidence of BR requiring intervention (BRRI) and its highly correlated factors.
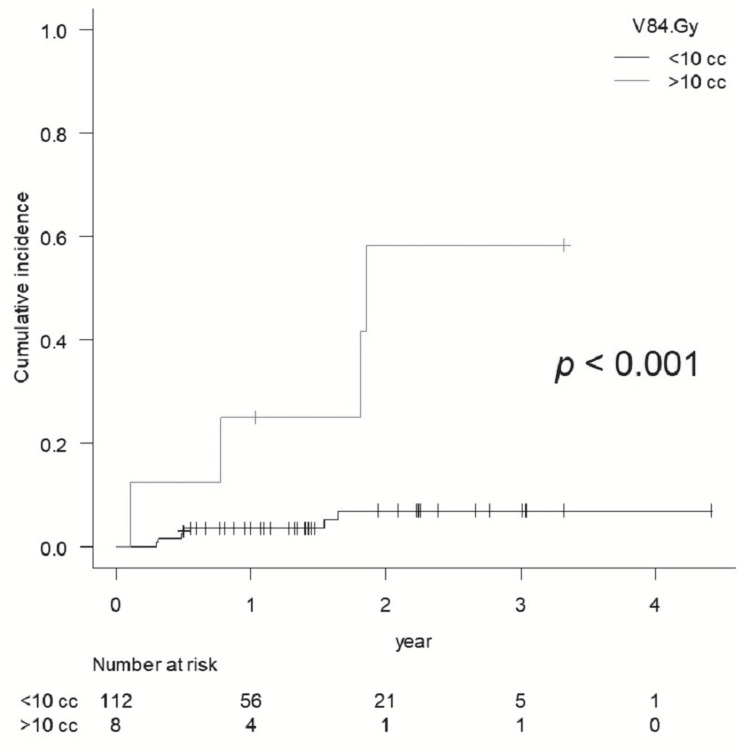
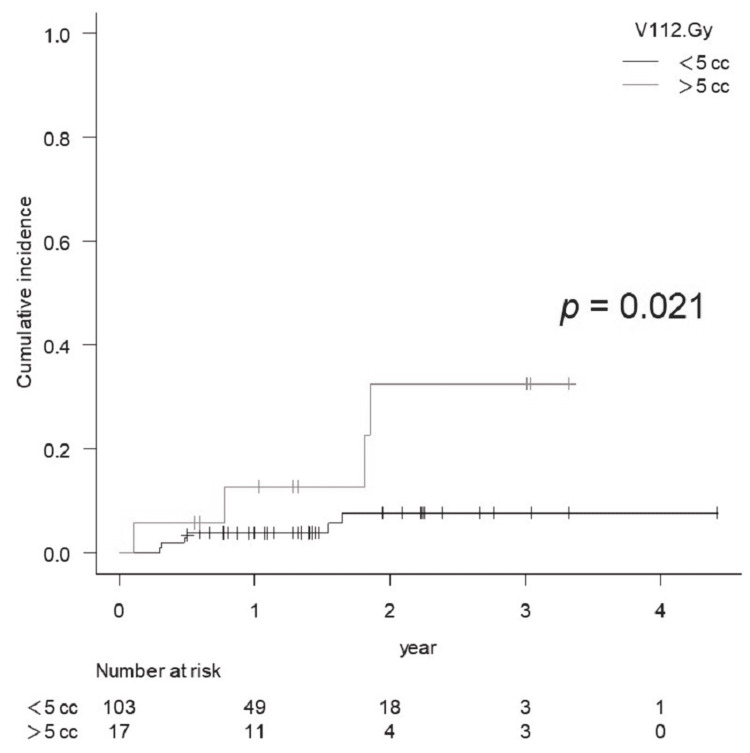
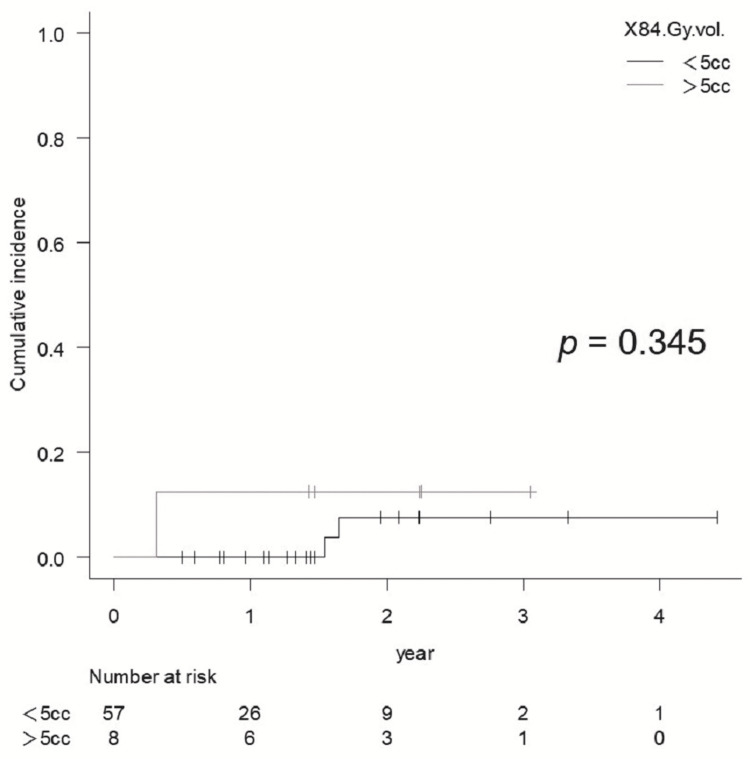
Patients with BMs treated with sSRS or fSRS using Vero4DRT at Toyohashi Municipal Hospital between July 2017 and June 2021 were retrospectively reviewed, of whom patients were available for at least 20 weeks of magnetic resonance imaging follow-up from SRS were included, and analyzed. The prescribed dose fractionation schemes to the planning target volume (PTV) boundary included 24 Gy (sSRS), 35 Gy (5 fractions [fr]), 42 Gy (10 fr), and 30 Gy (3 fr), according to the tumor volume and location. The volume of the surrounding normal brain receiving 84 Gy (V84 Gy, biologically effective dose [BED] based on a linear-quadratic model with an alpha/beta ratio of 2, single-dose equivalent [SDE] to 12 Gy), V112 Gy (BED, SDE to 14 Gy) for all lesions, and all irradiated volume, including gross tumor volume (GTV) receiving 81.6 Gy (81.6 Gy vol., BED) for fSRS were calculated, for which cerebrospinal fluid and bone volumes were cautiously excluded. The diagnosis of tumor progression or BR dominance was based on serial T1/T2 matching.
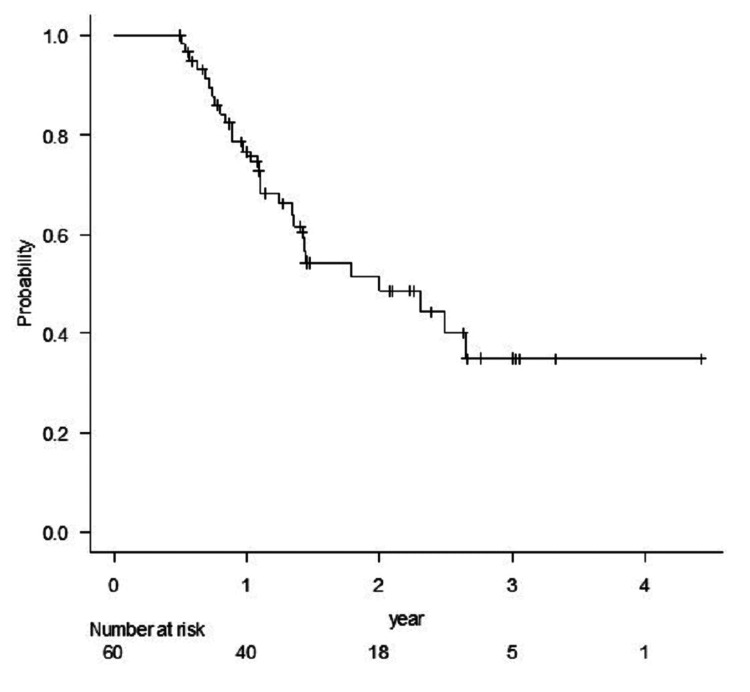
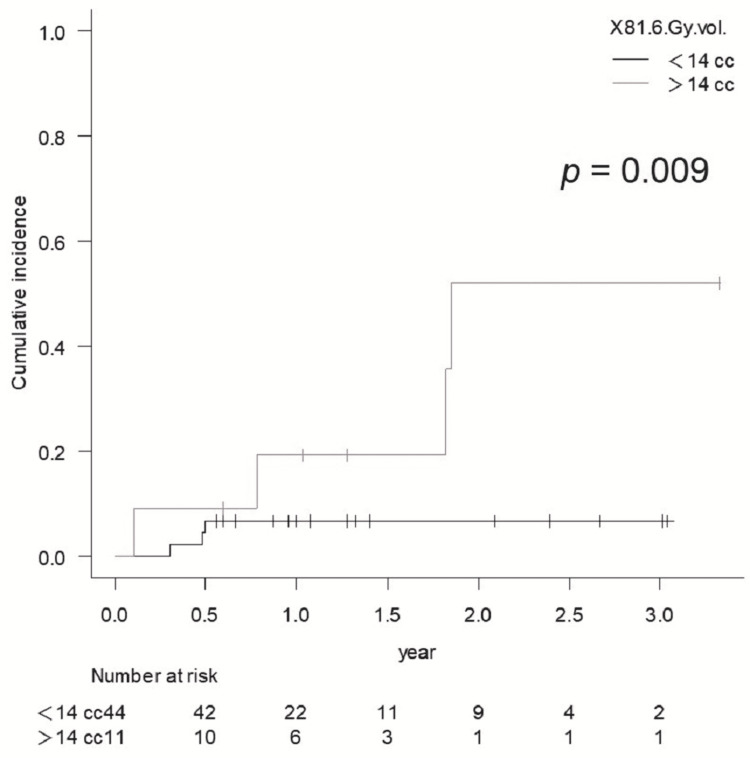
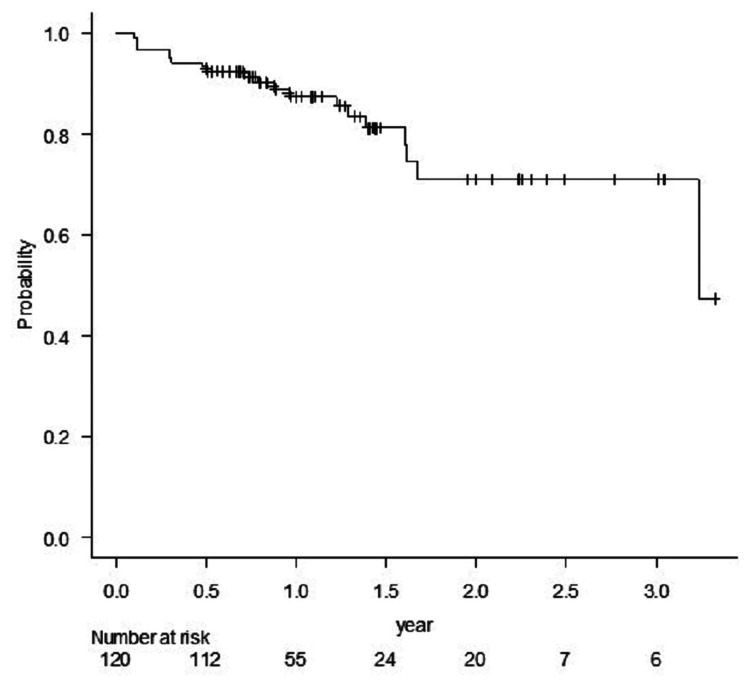
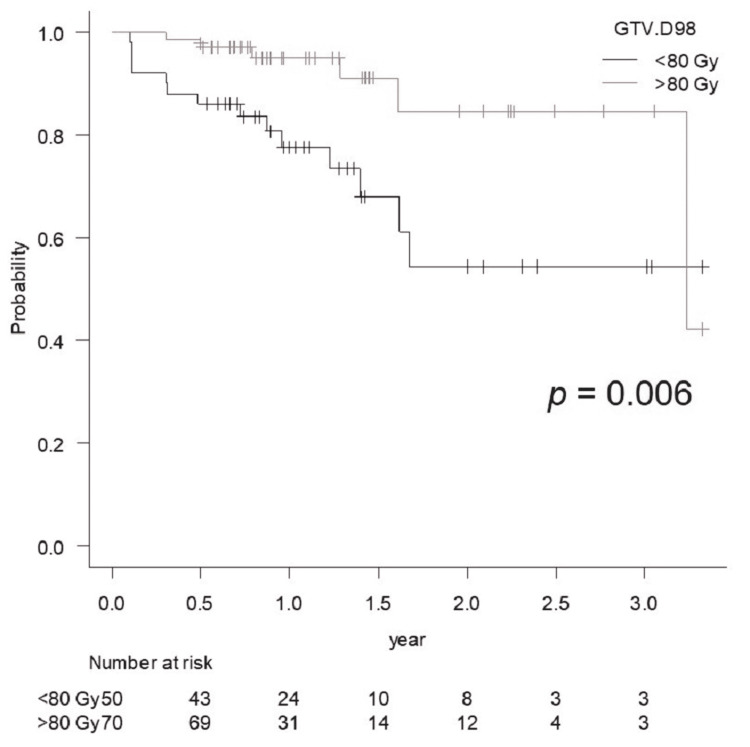
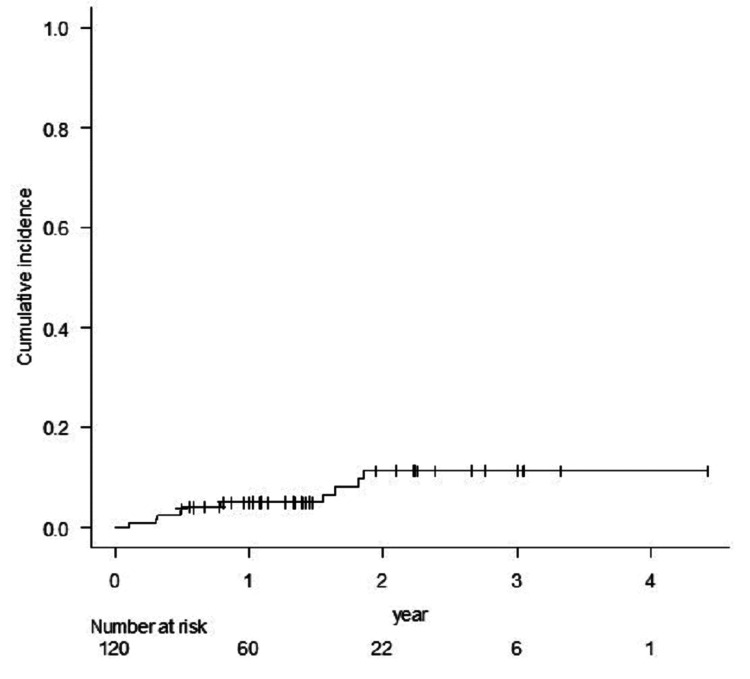
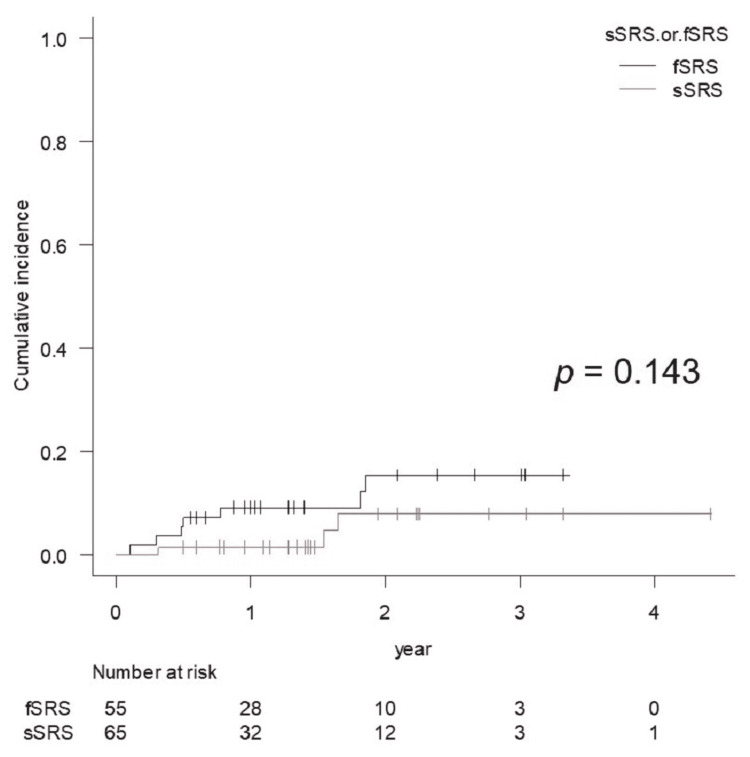
Sixty patients with 120 lesions (65 treated with sSRS and 55 treated with fSRS) were included in the final analysis, with a median follow-up period of 65 weeks. The local control rate at one year was 87.5%. The cumulative incidence of BRRI within two years was 11.5%. The risk of symptomatic BR was significantly higher for V84 Gy >10 cc ( <0.001) and V112 Gy >5 cc ( = 0.021). In the fSRS group, the cumulative incidence of Grade 3 BR and those requiring resection was significantly higher for 81.6 Gy vol. >14 cc ( = 0.003 and = 0.004, respectively). The coexistence of viable tumor tissue and BR could not be ruled out for enlarging lesions after the nadir response, especially for fSRS, due to a lower BED to GTV margin (<80 Gy, BED).
Stereotactic irradiation with Vero4DRT provided efficacy and safety comparable to previous linear accelerator series, and most of the dose-volume thresholds for BRRI presented in this study were notably lower than those reported in previous studies. This study suggests that the indication of single and up to 5 frSRS should be limited to far smaller tumors than previously acknowledged to ensure long-term safety and efficacy.
迄今为止,已有多项因素被报道与脑转移瘤(BM)单次或分次立体定向放射外科治疗(sSRS或fSRS)后脑放射性坏死(BR)相关,包括接受特定剂量的周围脑体积;然而,这些因素,尤其是fSRS相关因素,尚未完全阐明。此外,使用Vero4DRT进行SRS治疗的BM患者的临床结局数据极为有限。因此,本研究旨在阐明需要干预的BR(BRRI)的发生率及其高度相关因素。
回顾性分析2017年7月至2021年6月在丰桥市立医院接受使用Vero4DRT的sSRS或fSRS治疗的BM患者,纳入SRS后至少有20周磁共振成像随访资料的患者并进行分析。根据肿瘤体积和位置,计划靶体积(PTV)边界的处方剂量分割方案包括24 Gy(sSRS)、35 Gy(5次分割[fr])、42 Gy(10 fr)和30 Gy(3 fr)。计算所有病灶接受84 Gy(V84 Gy,基于α/β比值为2的线性二次模型的生物等效剂量[BED],单次剂量等效[SDE]至12 Gy)、V112 Gy(BED,SDE至14 Gy)的周围正常脑体积,以及fSRS中接受81.6 Gy(81.6 Gy体积,BED)的包括大体肿瘤体积(GTV)在内的所有照射体积,计算时谨慎排除脑脊液和骨体积。肿瘤进展或BR占优的诊断基于连续T1/T2匹配。
最终分析纳入60例患者的120个病灶(65例接受sSRS治疗,55例接受fSRS治疗),中位随访期为65周。一年时的局部控制率为87.5%。两年内BRRI的累积发生率为11.5%。V84 Gy>10 cc(<0.001)和V112 Gy>5 cc(=0.021)时,有症状BR的风险显著更高。在fSRS组中,81.6 Gy体积>14 cc时,3级BR和需要切除的BR的累积发生率显著更高(分别为=0.003和=0.004)。由于GTV边缘的BED较低(<80 Gy,BED),在最低点反应后病灶增大时,不能排除存活肿瘤组织与BR并存,尤其是fSRS。
使用Vero4DRT进行立体定向照射提供了与先前直线加速器系列相当的疗效和安全性,本研究中提出的大多数BRRI剂量体积阈值明显低于先前研究报道的值。本研究表明,单次和最多5次分割的SRS的适应证应限于比先前公认的小得多的肿瘤,以确保长期安全性和疗效。