Ohtakara Kazuhiro, Arakawa Sosuke, Nakao Makoto, Muramatsu Hideki, Suzuki Kojiro
Department of Radiation Oncology, Kainan Hospital Aichi Prefectural Welfare Federation of Agricultural Cooperatives, Yatomi, JPN.
Department of Radiology, Aichi Medical University, Nagakute, JPN.
Cureus. 2023 Aug 31;15(8):e44492. doi: 10.7759/cureus.44492. eCollection 2023 Aug.
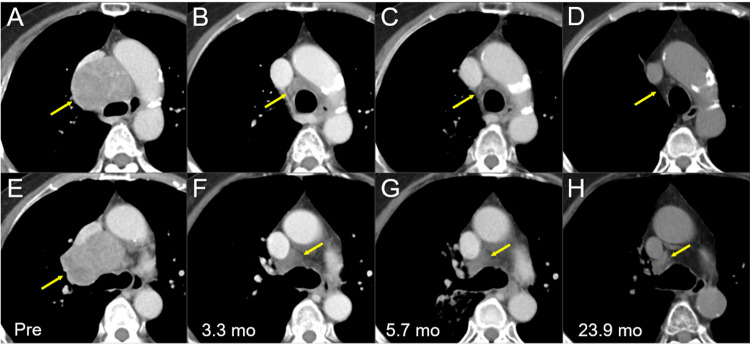
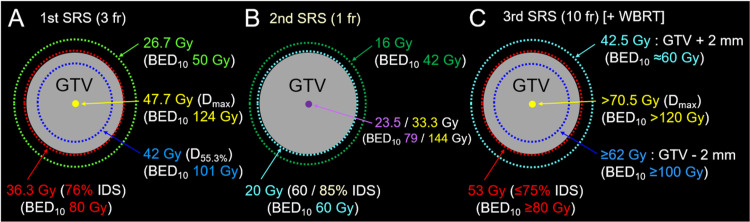
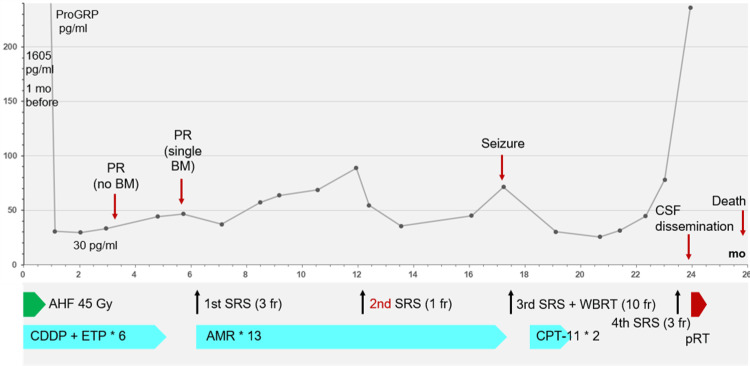
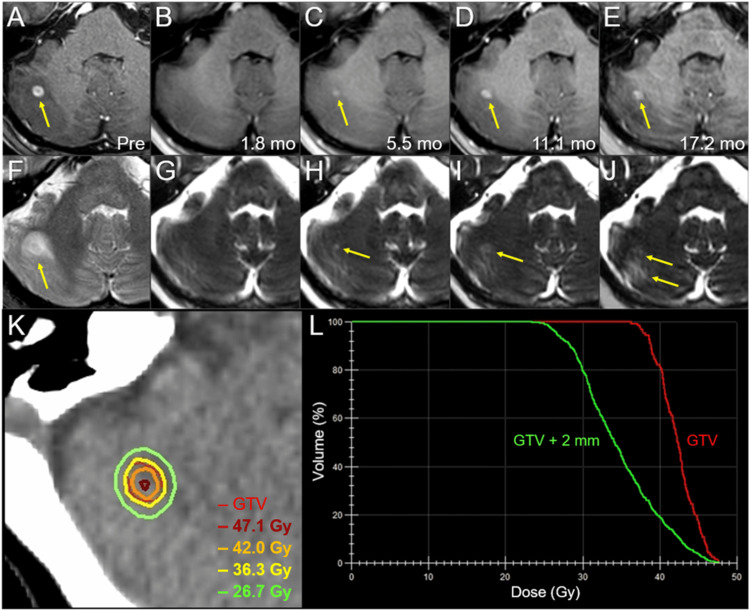
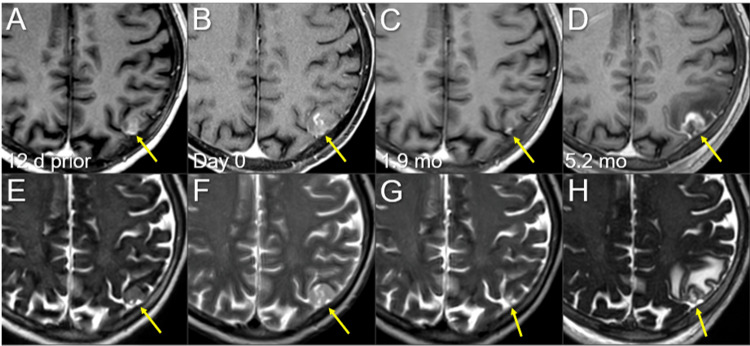
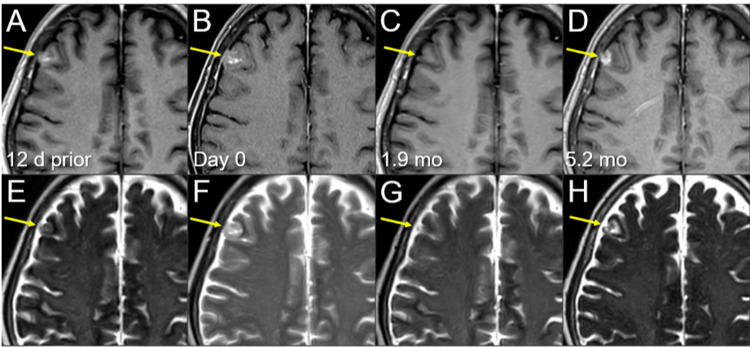
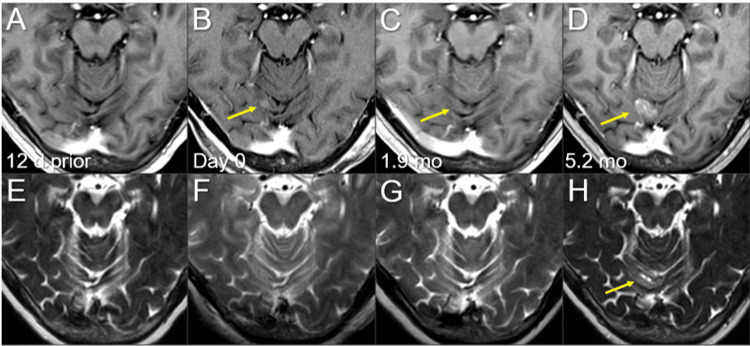
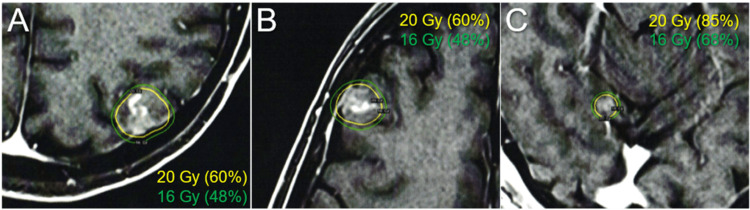
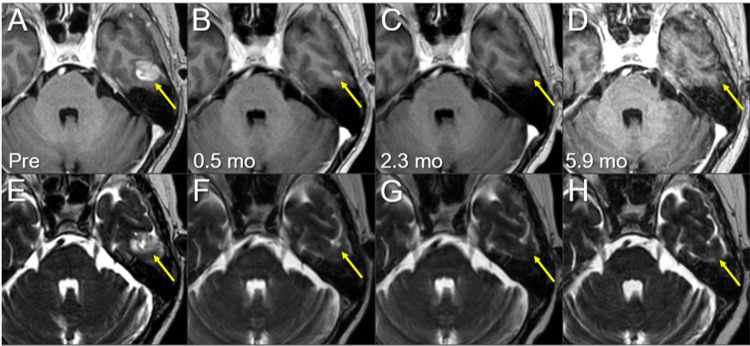
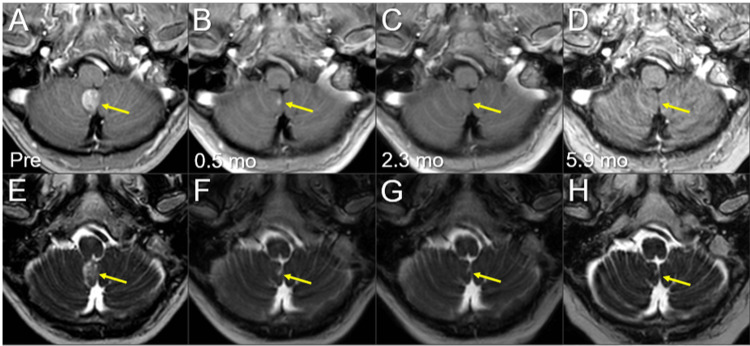
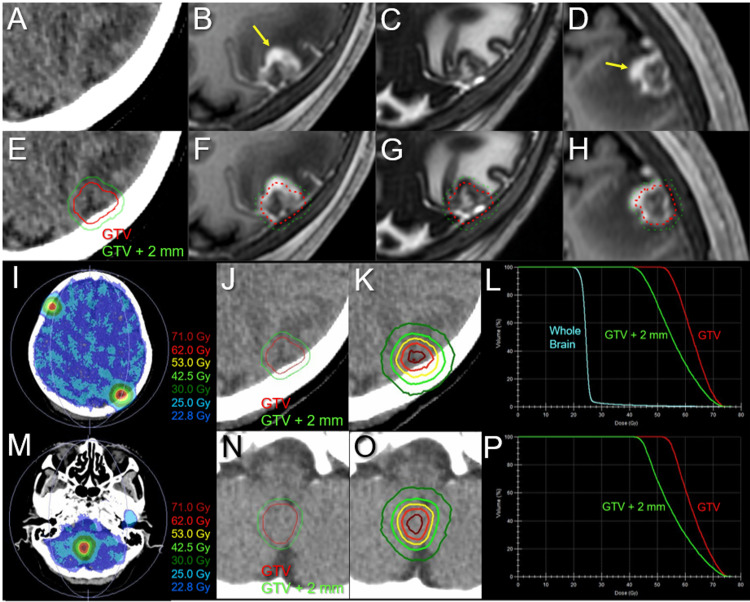
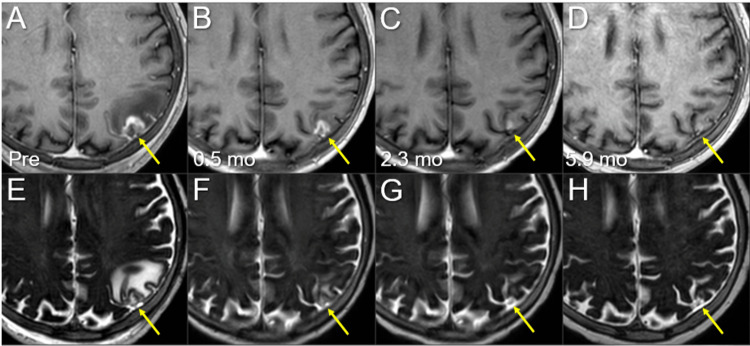
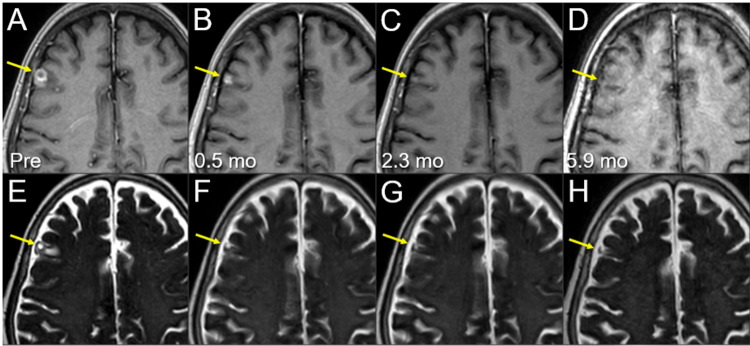
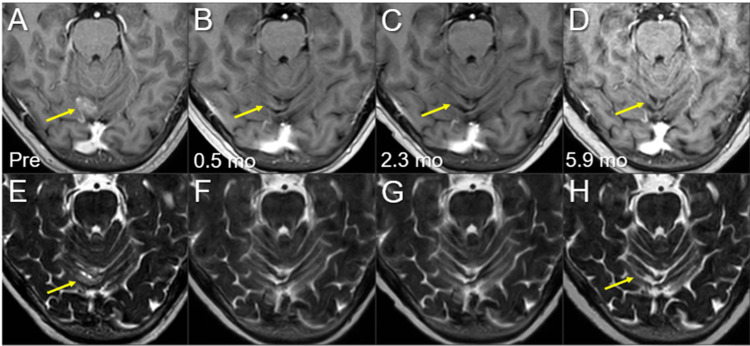
First-line and possibly repeated stereotactic radiosurgery (SRS) with preserving whole-brain radiotherapy (WBRT) is an attractive and promising option for synchronous or metachronous limited brain metastases (BMs) from small cell lung cancer (SCLC), for which a modest prescription dose is generally preferred, such as a biological effective dose of ≤60 Gy, based on the linear-quadratic formula with an alpha/beta ratio of 10 (BED). In addition, the optimal planning scheme for re-SRS for local progression after SRS of BMs from SCLC remains unclear. Herein, we describe a case of limited BMs developing after a partial response to standard chemoradiotherapy (CRT) for limited-stage SCLC. The BMs, including local failures following prior single-fraction (fr) SRS, were re-treated with volumetric-modulated arc-based SRS combined with simultaneous reduced-dose WBRT. The first SRS with 36.3 Gy/3 fr (BED 80 Gy) for a small BM resulted in a local control of 17.2 months. However, the second SRS with 20 Gy/1 fr (BED 60 Gy) to the 60% or 85% isodose surface (IDS) covering the gross tumor volume (GTV) of three new BMs with a paradoxical T1/T2 mismatch, that is, a visible mass on T2 larger than an enhancing area, resulted in partial symptomatic local progression of all lesions within 5.2 months, along with the development of two new lesions, despite continued amrubicin monotherapy. In contrast, the third SRS with 53 Gy/10 fr (BED 81 Gy) to ≤74% IDSs encompassing the GTV boundary resulted in complete responses of all the lesions during six months. However, despite a combined use of WBRT of 25 Gy in the third SRS, symptomatic spinal cerebrospinal fluid dissemination and new BMs developed, the former leading to patient mortality. A BED of ≥80 Gy to the GTV margin and a steep dose increase inside the GTV boundary are suitable to ensure excellent local control in SRS for SCLC BMs. Re-SRS with the aforementioned scheme can be an efficacious option for local failures following prior SRS with a BED of ≤60 Gy. Modest dose escalation with a simultaneous integrated boost to bulky lesions in the initial CRT may reduce the development of new BM through improved control of the potential source.
对于小细胞肺癌(SCLC)的同步或异时性局限性脑转移瘤(BMs),一线且可能重复进行的立体定向放射外科治疗(SRS)并保留全脑放疗(WBRT)是一种有吸引力且有前景的选择,对于这种情况,基于α/β比值为10的线性二次公式(生物等效剂量,BED),通常更倾向于适度的处方剂量,例如生物等效剂量≤60 Gy。此外,SCLC的BMs在SRS后局部进展的再程SRS的最佳计划方案仍不清楚。在此,我们描述了一例在局限期SCLC的标准放化疗(CRT)部分缓解后出现局限性BMs的病例。这些BMs,包括先前单次分割(fr)SRS后的局部复发,采用基于容积调强弧形放疗的SRS联合同步减量WBRT进行再治疗。对一个小的BM进行的首次SRS,剂量为36.3 Gy/3 fr(BED 80 Gy),实现了17.2个月的局部控制。然而,对三个新的BMs的大体肿瘤体积(GTV)进行的第二次SRS,剂量为20 Gy/1 fr(BED 60 Gy),照射60%或85%等剂量面(IDS),出现了矛盾的T1/T2不匹配,即T2上可见的肿块大于强化区域,导致所有病灶在5.2个月内出现部分有症状的局部进展,同时出现了两个新病灶,尽管继续使用氨柔比星单药治疗。相比之下,对包含GTV边界的≤74% IDS进行的第三次SRS,剂量为53 Gy/10 fr(BED 81 Gy),导致所有病灶在6个月内完全缓解。然而,尽管在第三次SRS中联合使用了25 Gy的WBRT,但仍出现了有症状的脊髓脑脊液播散和新的BMs,前者导致患者死亡。对GTV边缘给予≥80 Gy的BED以及在GTV边界内陡峭的剂量增加,适合确保SCLC的BMs在SRS中实现良好的局部控制。采用上述方案的再程SRS对于先前BED≤60 Gy的SRS后的局部复发可能是一种有效的选择。在初始CRT中对大体积病灶进行适度的剂量递增并同时进行整合加量,可能通过改善对潜在源头的控制来减少新BMs的发生。