Balcar Lorenz, Tonon Marta, Semmler Georg, Calvino Valeria, Hartl Lukas, Incicco Simone, Jachs Mathias, Bauer David, Hofer Benedikt Silvester, Gambino Carmine Gabriele, Accetta Antonio, Brocca Alessandra, Trauner Michael, Mandorfer Mattias, Piano Salvatore, Reiberger Thomas
Division of Gastroenterology and Hepatology, Department of Internal Medicine III, Medical University of Vienna, Vienna, Austria.
Vienna Hepatic Hemodynamic Lab, Division of Gastroenterology and Hepatology, Department of Internal Medicine III, Medical University of Vienna, Vienna, Austria.
JHEP Rep. 2022 Jun 3;4(8):100513. doi: 10.1016/j.jhepr.2022.100513. eCollection 2022 Aug.
BACKGROUND & AIMS: Although ascites is the most frequent first decompensating event in cirrhosis, the clinical course after ascites as the index decompensation is not well defined. The aim of this multicentre study was thus to systematically investigate the incidence and type of further decompensation after ascites as the first decompensating event and to assess risk factors for mortality.
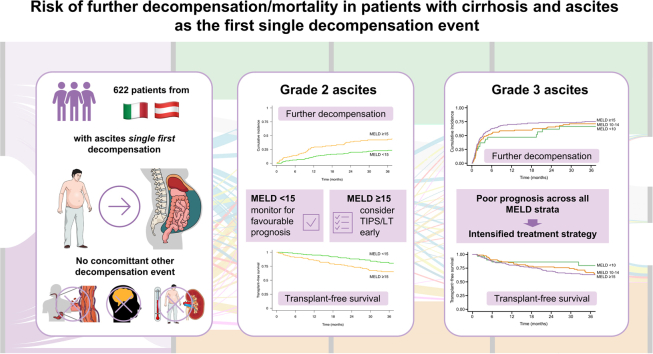
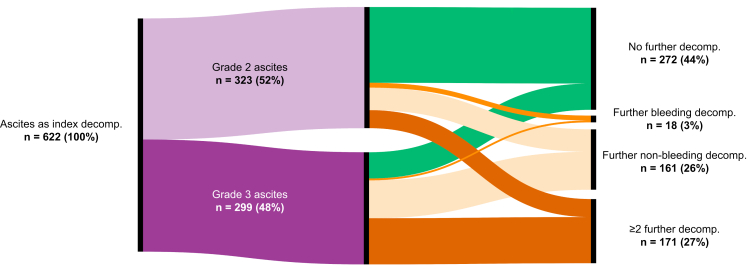
A total of 622 patients with cirrhosis presenting with grade 2/3 ascites as the index decompensating event at 2 university hospitals (Padova and Vienna) between 2003 and 2021 were included. Events of further decompensation, liver transplantation, and death were recorded.
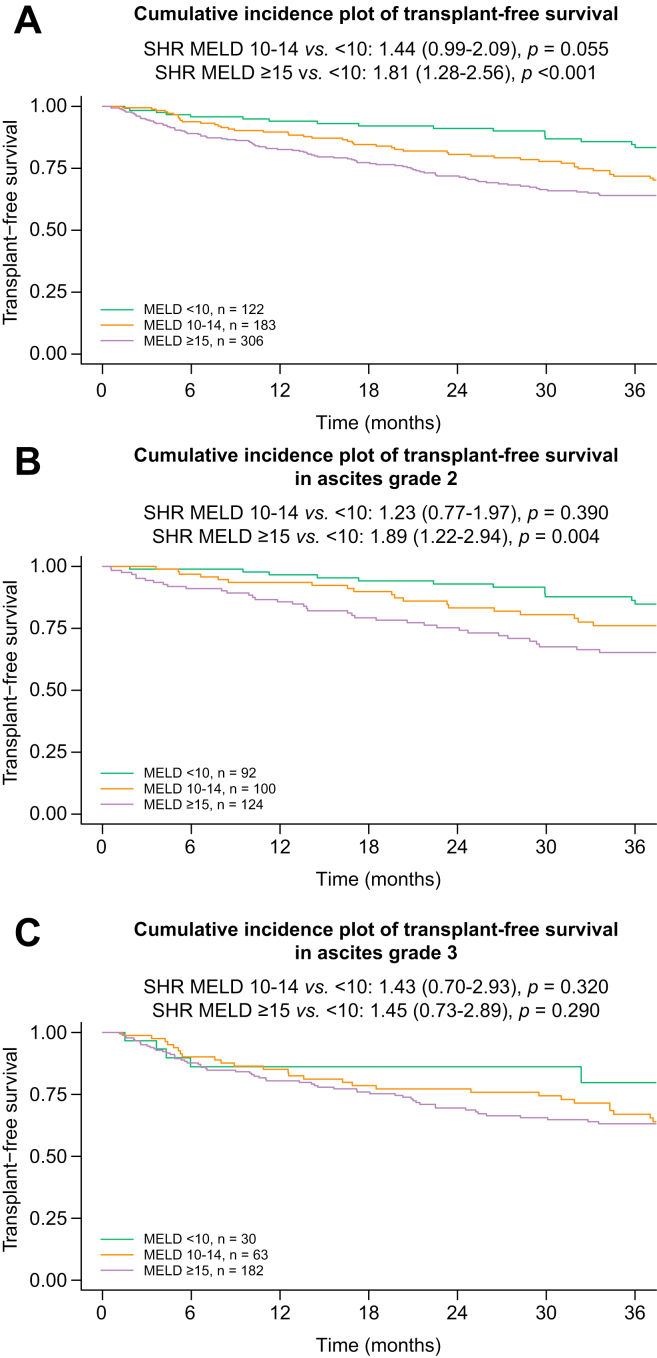
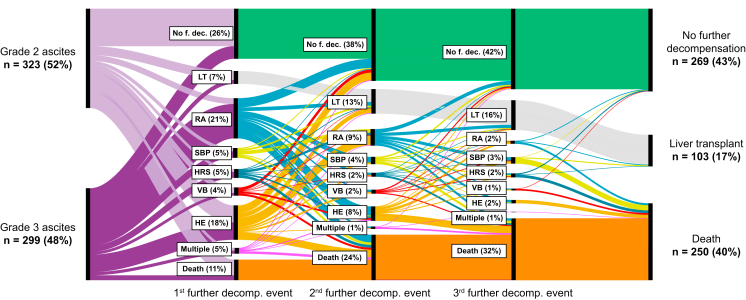
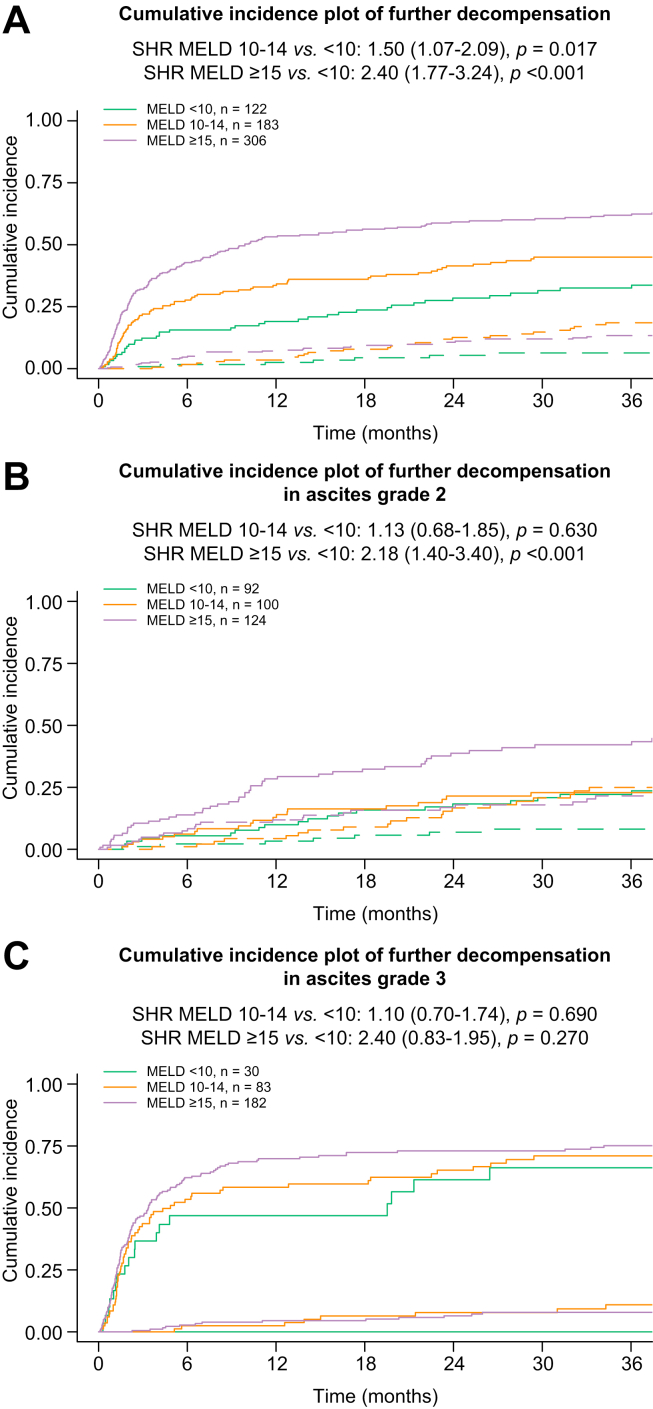
The mean age was 57 ± 11 years, and most patients were male (n = 423, 68%) with alcohol-related (n = 366, 59%) and viral (n = 200,32%) liver disease as the main aetiologies. In total, 323 (52%) patients presented with grade 2 and 299 (48%) with grade 3 ascites. The median Child-Pugh score at presentation was 8 (IQR 7-9), and the mean model for end-stage liver disease (MELD) was 15 ± 6. During a median follow-up period of 49 months, 350 (56%) patients experienced further decompensation: refractory ascites (n = 130, 21%), hepatic encephalopathy (n = 112, 18%), spontaneous bacterial peritonitis (n = 32, 5%), hepatorenal syndrome-acute kidney injury (n = 29, 5%). Variceal bleeding as an isolated further decompensation event was rare (n = 18, 3%), whereas non-bleeding further decompensation (n = 161, 26%) and ≥2 concomitant further decompensation events (n = 171, 27%) were frequent. Transjugular intrahepatic portosystemic shunt was used in only 81 (13%) patients. In patients presenting with grade 2 ascites, MELD ≥15 indicated a considerable risk for further decompensation (subdistribution hazard ratio [SHR] 2.18; <0.001; 1-year incidences: <10: 10% . 10-14: 13% . ≥15: 28%) and of mortality (SHR 1.89; = 0.004; 1-year incidences: <10: 3% . 10-14: 6% vs. ≥15: 14%). Importantly, mortality was similarly high throughout MELD strata in grade 3 ascites ( = n.s. for different MELD strata; 1-year incidences: <10: 14% 10-14: 15% . ≥15: 20%).
Further decompensation is frequent in patients with ascites as a index decompensation event and only rarely owing to bleeding. Although patients with grade 2 ascites and MELD <15 seem to have a favourable prognosis, those with grade 3 ascites are at a high risk of mortality across all MELD strata.
Decompensation (the development of symptoms as a result of worsening liver function) marks a turning point in the disease course for patients with cirrhosis. Ascites ( the accumulation of fluid in the abdomen) is the most common first decompensating event, yet little is known about the clinical course of patients who develop ascites as a first decompensating event. Herein, we show that the severity of ascites is associated with mortality and that in patients with moderate ascites, the widely used prognostic MELD score can predict patient outcomes.
尽管腹水是肝硬化最常见的首次失代偿事件,但以腹水作为首次失代偿事件后的临床病程尚不明确。因此,这项多中心研究的目的是系统地调查以腹水作为首次失代偿事件后进一步失代偿的发生率和类型,并评估死亡的危险因素。
纳入2003年至2021年间在2家大学医院(帕多瓦和维也纳)以2/3级腹水作为首次失代偿事件的622例肝硬化患者。记录进一步失代偿、肝移植和死亡事件。
平均年龄为57±11岁,大多数患者为男性(n=423,68%),主要病因是酒精性肝病(n=366,59%)和病毒性肝病(n=200,32%)。总共323例(52%)患者为2级腹水,299例(48%)为3级腹水。就诊时Child-Pugh评分中位数为8(四分位间距7-9),终末期肝病模型(MELD)平均评分为15±6。在中位随访期49个月内,350例(56%)患者发生了进一步失代偿:顽固性腹水(n=130,21%)、肝性脑病(n=112,18%)、自发性细菌性腹膜炎(n=32,5%)、肝肾综合征急性肾损伤(n=29,5%)。孤立性静脉曲张破裂出血作为进一步失代偿事件很少见(n=18,3%),而非出血性进一步失代偿(n=161,26%)和≥2种并发进一步失代偿事件(n=171,27%)很常见,仅81例(13%)患者使用了经颈静脉肝内门体分流术。在2级腹水患者中,MELD≥15表明进一步失代偿风险相当高(亚分布风险比[SHR]2.18;P<0.001;1年发生率:<10:10%,10-14:13%,≥15:28%)和死亡风险高(SHR1.89;P=0.004;1年发生率:<10:3%,10-14:6%,≥15:14%)。重要的是,3级腹水患者在所有MELD分层中的死亡率同样很高(不同MELD分层P值无统计学意义;1年发生率:<10:14%,10-14:15%,≥15:20%)。
以腹水作为首次失代偿事件后的进一步失代偿很常见,且很少由出血引起。尽管2级腹水且MELD<15的患者似乎预后良好,但3级腹水患者在所有MELD分层中均有较高的死亡风险。
失代偿(由于肝功能恶化而出现症状)标志着肝硬化患者疾病进程的转折点。腹水(腹部积液)是最常见的首次失代偿事件,但对于以腹水作为首次失代偿事件的患者的临床病程知之甚少。在此,我们表明腹水的严重程度与死亡率相关,并且在中度腹水患者中,广泛使用的预后指标MELD评分可以预测患者的预后。