National Immunization Program, Chinese Center for Disease Control and Prevention, Beijing, People's Republic of China.
Henan Provincial Disease Control and Prevention, People's Republic of China, Henan.
Emerg Microbes Infect. 2022 Dec;11(1):1950-1958. doi: 10.1080/22221751.2022.2103455.
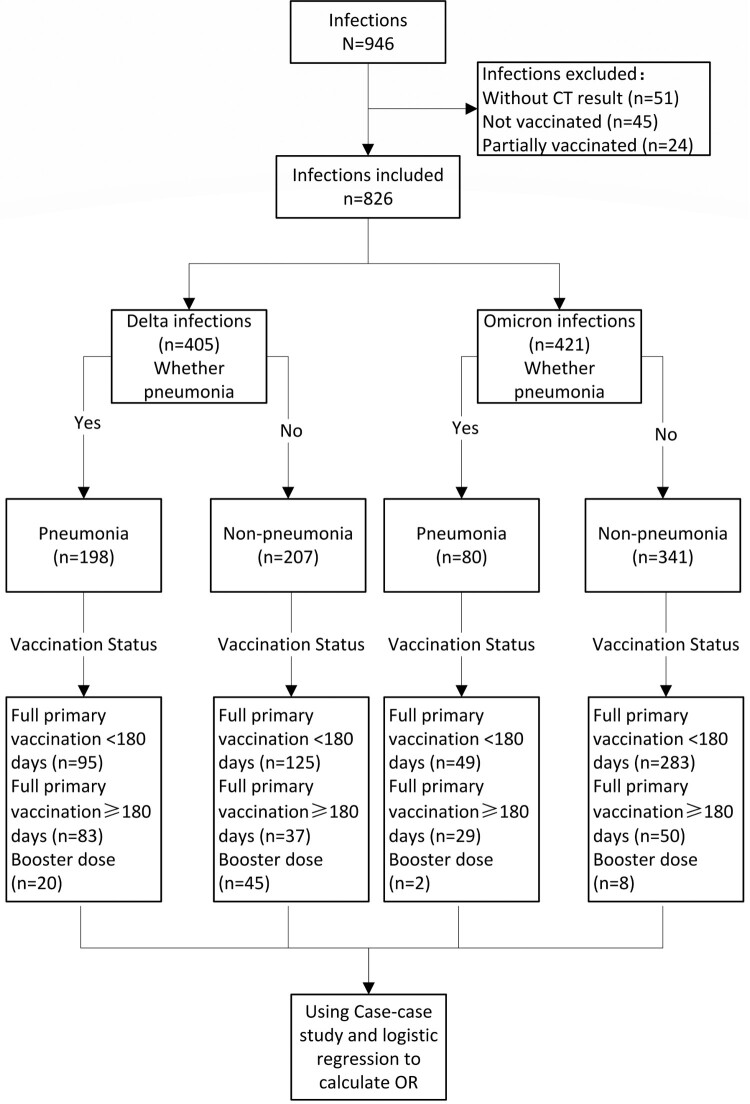
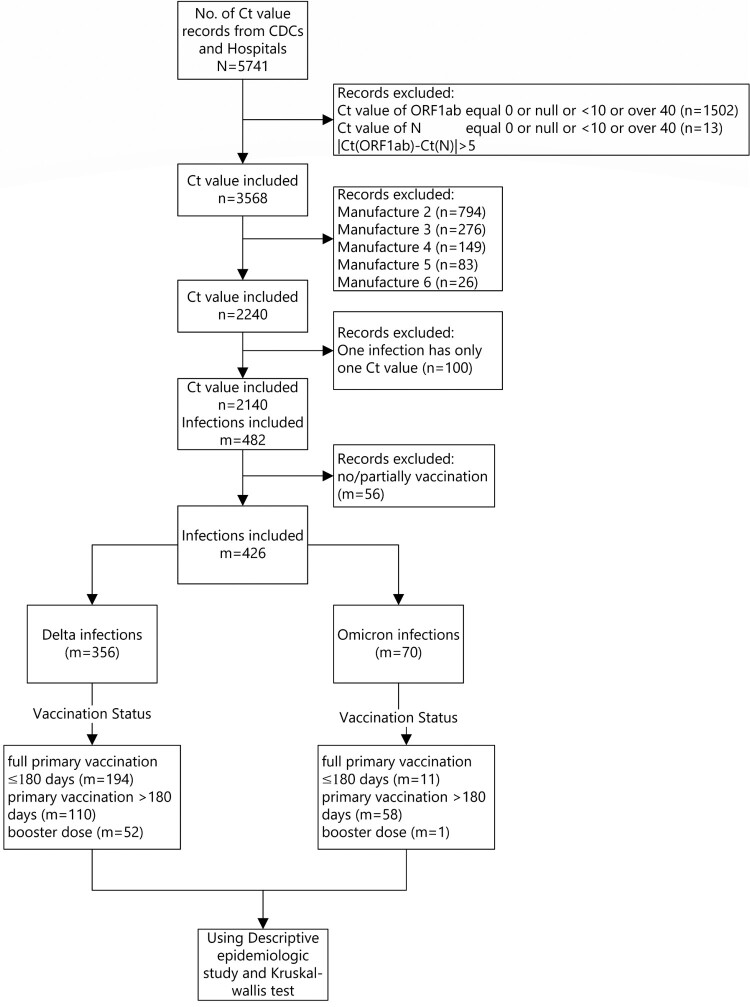
Using a three-prefecture, two-variant COVID-19 outbreak in Henan province in January 2022, we evaluated the associations of primary and booster immunization with China-produced COVID-19 vaccines and COVID-19 pneumonia and SARS-CoV-2 viral load among persons infected by Delta or Omicron variant. We obtained demographic, clinical, vaccination, and multiple Ct values of infections ≥3 years of age. Vaccination status was either primary series ≥180 days prior to infection; primary series <180 days prior to infection, or booster dose recipient. We used logistic regression to determine odds ratios (OR) of Delta and Omicron COVID-19 pneumonia by vaccination status. We analysed minimum Ct values by vaccination status, age, and variant. Of 826 eligible cases, 405 were Delta and 421 were Omicron cases; 48.9% of Delta and 19.0% of Omicron cases had COVID-19 pneumonia. Compared with full primary vaccination ≥180 days before infection, the aOR of pneumonia was 0.48 among those completing primary vaccination <180 days and 0.18 among booster recipients among these Delta infections. Among Omicron infections, the corresponding aOR was 0.34 among those completing primary vaccination <180 days. There were too few (ten) Omicron cases among booster dose recipients to calculate a reliable OR. There were no differences in minimum Ct values by vaccination status among the 356 Delta cases or 70 Omicron cases. COVID-19 pneumonia was less common among Omicron cases than Delta cases. Full primary vaccination reduced pneumonia effectively for 6 months; boosting six months after primary vaccination resulted in further reduction. We recommend accelerating the pace of booster dose administration.
利用 2022 年 1 月河南省三省两区的 COVID-19 暴发,我们评估了原发性和加强免疫接种与中国生产的 COVID-19 疫苗以及德尔塔或奥密克戎变异株感染者的 COVID-19 肺炎和 SARS-CoV-2 病毒载量之间的关联。我们获得了≥3 岁人群的人口统计学、临床、疫苗接种和多次感染 Ct 值。接种状态为感染前≥180 天的初级系列;感染前<180 天的初级系列或加强剂量接受者。我们使用逻辑回归来确定 Delta 和 Omicron COVID-19 肺炎的接种状态的优势比(OR)。我们按接种状态、年龄和变异体分析了最小 Ct 值。在 826 例合格病例中,405 例为 Delta 病例,421 例为 Omicron 病例;48.9%的 Delta 病例和 19.0%的 Omicron 病例患有 COVID-19 肺炎。与感染前≥180 天完成全初级疫苗接种相比,在 Delta 感染中,<180 天完成初级疫苗接种者的肺炎的 aOR 为 0.48,而加强剂接受者的 aOR 为 0.18。在 Omicron 感染中,<180 天完成初级疫苗接种者的相应 aOR 为 0.34。加强剂量接受者中 Omicron 病例太少(10 例),无法计算可靠的 OR。在 356 例 Delta 病例或 70 例 Omicron 病例中,疫苗接种状态与最小 Ct 值之间没有差异。Omicron 病例的肺炎比 Delta 病例少见。全初级疫苗接种在 6 个月内有效地减少了肺炎;在初级疫苗接种后 6 个月加强疫苗接种会进一步降低肺炎的风险。我们建议加快加强剂量接种的速度。