Institute of Health Informatics, University College London, London, UK.
Institute for Global Health, University College London, London, UK.
Lancet Healthy Longev. 2022 May;3(5):e347-e355. doi: 10.1016/S2666-7568(22)00093-9. Epub 2022 May 4.
The SARS-CoV-2 omicron variant (B.1.1.529) is highly transmissible, but disease severity appears to be reduced compared with previous variants such as alpha and delta. We investigated the risk of severe outcomes following infection in residents of long-term care facilities.
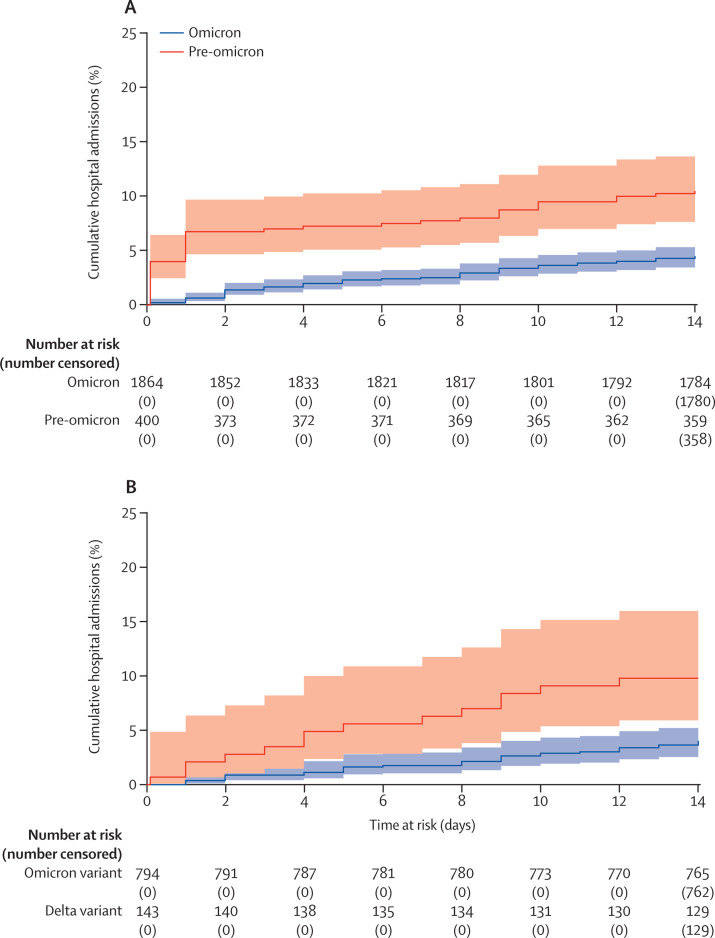
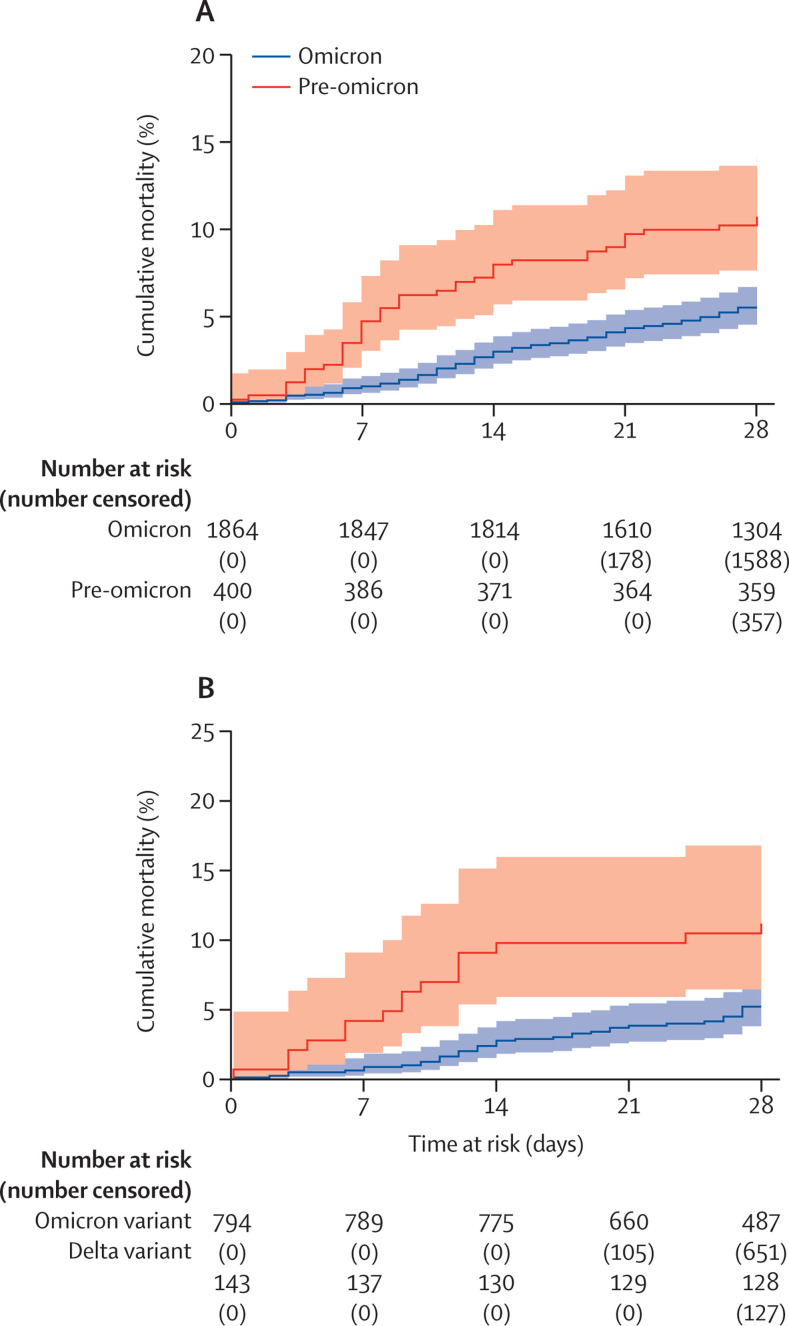
We did a prospective cohort study in residents of long-term care facilities in England who were tested regularly for SARS-CoV-2 between Sept 1, 2021, and Feb 1, 2022, and who were participants of the VIVALDI study. Residents were eligible for inclusion if they had a positive PCR or lateral flow device test during the study period, which could be linked to a National Health Service (NHS) number, enabling linkage to hospital admissions and mortality datasets. PCR or lateral flow device test results were linked to national hospital admission and mortality records using the NHS-number-based pseudo-identifier. We compared the risk of hospital admission (within 14 days following a positive SARS-CoV-2 test) or death (within 28 days) in residents who had tested positive for SARS-CoV-2 in the period shortly before omicron emerged (delta-dominant) and in the omicron-dominant period, adjusting for age, sex, primary vaccine course, past infection, and booster vaccination. Variants were confirmed by sequencing or spike-gene status in a subset of samples.
795 233 tests were done in 333 long-term care facilities, of which 159 084 (20·0%) could not be linked to a pseudo-identifier and 138 012 (17·4%) were done in residents. Eight residents had two episodes of infection (>28 days apart) and in these cases the second episode was excluded from the analysis. 2264 residents in 259 long-term care facilities (median age 84·5 years, IQR 77·9-90·0) were diagnosed with SARS-CoV-2, of whom 253 (11·2%) had a previous infection and 1468 (64·8%) had received a booster vaccination. About a third of participants were male. Risk of hospital admissions was markedly lower in the 1864 residents infected in the omicron-period (4·51%, 95% CI 3·65-5·55) than in the 400 residents infected in the pre-omicron period (10·50%, 7·87-13·94), as was risk of death (5·48% [4·52-6·64] 10·75% [8·09-14·22]). Adjusted hazard ratios (aHR) also indicated a reduction in hospital admissions (0·64, 95% CI 0·41-1·00; p=0·051) and mortality (aHR 0·68, 0·44-1·04; p=0·076) in the omicron versus the pre-omicron period. Findings were similar in residents with a confirmed variant.
Observed reduced severity of the omicron variant compared with previous variants suggests that the wave of omicron infections is unlikely to lead to a major surge in severe disease in long-term care facility populations with high levels of vaccine coverage or natural immunity. Continued surveillance in this vulnerable population is important to protect residents from infection and monitor the public health effect of emerging variants.
UK Department of Health and Social Care.
SARS-CoV-2 的奥密克戎变异株(B.1.1.529)具有高度传染性,但与阿尔法和德尔塔等先前的变异株相比,疾病的严重程度似乎有所降低。我们研究了长期护理机构居民感染后的严重后果风险。
我们在英格兰的长期护理机构居民中进行了一项前瞻性队列研究,他们在 2021 年 9 月 1 日至 2022 年 2 月 1 日期间定期接受 SARS-CoV-2 检测,并且是 VIVALDI 研究的参与者。如果居民在研究期间有阳性的 PCR 或侧向流动装置检测结果,且可以与国家卫生服务(NHS)号码相关联,从而可以与医院入院和死亡率数据集相关联,则符合纳入条件。使用基于 NHS 号码的伪标识符将 PCR 或侧向流动装置检测结果与国家医院入院和死亡率记录相关联。我们比较了在奥密克戎出现之前(delta 主导)和奥密克戎主导期间检测出 SARS-CoV-2 的居民在 14 天内(阳性 SARS-CoV-2 检测后)住院或死亡(28 天内)的风险,调整了年龄、性别、主要疫苗接种、既往感染和加强接种。通过测序或刺突基因状态在样本的亚集中确认了变体。
在 333 家长期护理机构中进行了 795233 次检测,其中 159084 次(20.0%)无法与伪标识符相关联,138012 次(17.4%)是在居民中进行的。8 名居民有两次感染(相隔>28 天),在这些情况下,第二次感染被排除在分析之外。在 259 家长期护理机构的 2264 名居民(中位年龄 84.5 岁,IQR 77.9-90.0)被诊断出患有 SARS-CoV-2,其中 253 名(11.2%)有既往感染,1468 名(64.8%)接受了加强接种。大约三分之一的参与者是男性。与 400 名在奥密克戎前感染的居民(10.50%,7.87-13.94)相比,在 1864 名在奥密克戎期感染的居民中,住院风险明显降低(4.51%,95%CI 3.65-5.55),死亡风险也是如此(5.48%[4.52-6.64] 10.75%[8.09-14.22])。调整后的危险比(aHR)也表明奥密克戎与前奥密克戎期相比,住院(0.64,95%CI 0.41-1.00;p=0.051)和死亡(0.68,0.44-1.04;p=0.076)的风险降低。在有确诊变异的居民中也发现了类似的结果。
与先前的变异株相比,观察到奥密克戎变异株的严重程度降低,这表明在疫苗接种率或自然免疫力较高的长期护理机构人群中,奥密克戎感染浪潮不太可能导致严重疾病的大幅增加。继续在这一脆弱人群中进行监测,对于保护居民免受感染和监测新出现的变异株对公共卫生的影响非常重要。
英国卫生部和社会保健部。