School of Mechanical Engineering, Iran University of Science and Technology, Tehran, Iran.
Foot & Ankle Research and Innovation Laboratory (FARIL), Department of Orthopaedic Surgery, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts, USA.
Orthop Surg. 2022 Sep;14(9):2238-2244. doi: 10.1111/os.13307. Epub 2022 Jul 19.
To determine whether unilateral chronic ankle instability (CAI) affects the kinematics of the uninjured contralateral ankle.
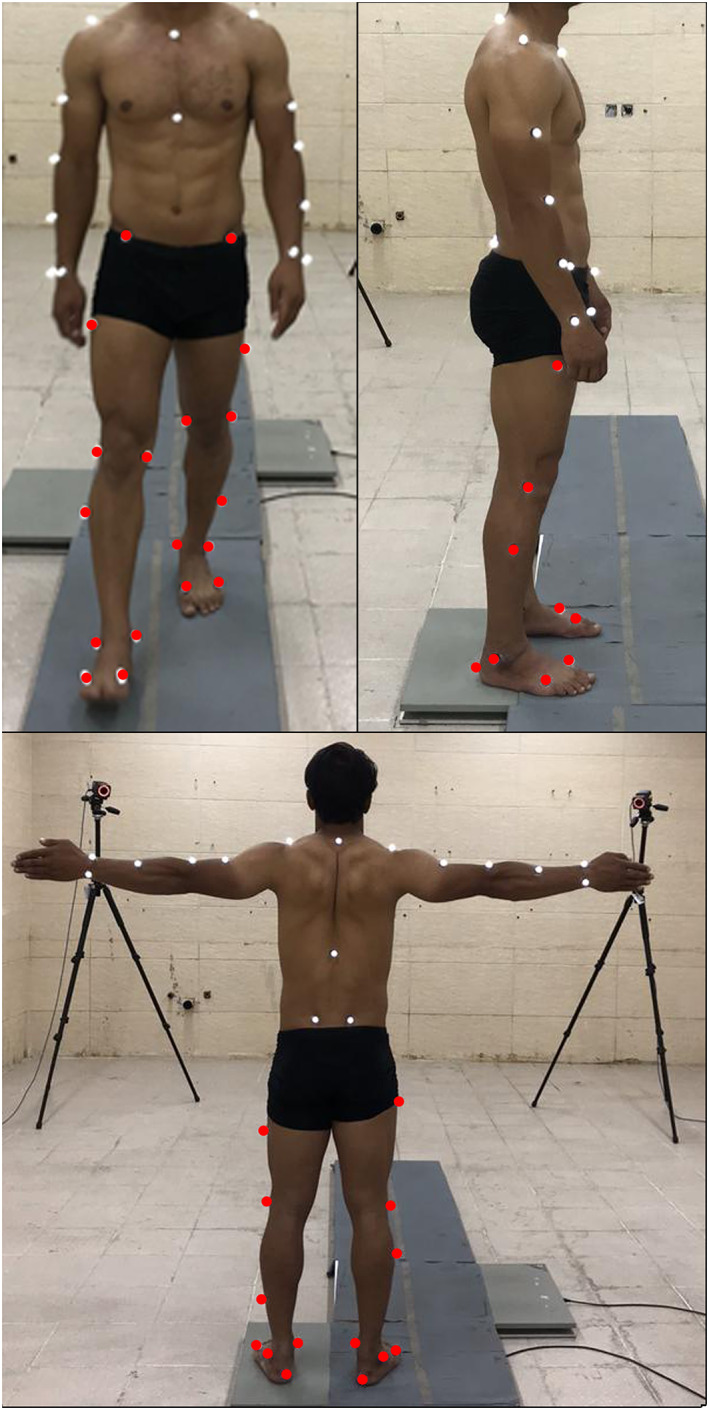
In this case-control study, 15 adult patients with unilateral CAI and 15 healthy controls were studied. Both the unstable and uninjured ankles in patients with unilateral CAI (CAI group, n = 15) were compared with that of healthy individuals (control group, n = 15). Applying body photo-reflective markers, the participant's motion during gait was measured. Biomechanical variables including overall ankle-toe angle, linear velocity, linear acceleration, angular velocity, angular acceleration, range of motion (RoM) in dorsiplantar flexion, and inversion-eversion at initial contact, loading response, mid-stance, terminal stance, pre-swing, and swing phase of the gait were measured.
In patients with CAI, the injured and uninjured ankles were significantly different regarding angle-toe angle, inversion-eversion RoM, dorsiplantar flexion in mid-stance, inversion-eversion at initial contact and terminal stance as well as the pre-swing and swing phases (p < 0.01). The uninjured ankles of patients showed lower ankle-toe velocity (p = 0.01) and acceleration (p = 0.01) compared to both the left and right ankles of the controls. In addition, the uninjured ankles of the patients showed decreased ankle dorsiflexion and increased inversion during initial contact, loading response, mid-stance, terminal stance, pre-swing, and swing compared to the control group (p < 0.017).
The results suggest that unilateral CAI can affect gait biomechanics in the contralateral uninjured ankle. Left unaddressed, unilateral CAI may lead to increased morbidity to the contralateral uninjured side. When surgery is not preferred for the management of unilateral CAI, rehabilitation protocols should focus on both sides.
确定单侧慢性踝关节不稳(CAI)是否会影响对侧未受伤踝关节的运动学。
在这项病例对照研究中,研究了 15 名单侧 CAI 成年患者和 15 名健康对照者。将单侧 CAI 患者的不稳定和未受伤踝关节(CAI 组,n=15)与健康个体(对照组,n=15)进行比较。应用身体反光标记物,测量参与者在步态中的运动。测量的生物力学变量包括整体踝关节-足角度、线性速度、线性加速度、角速度、角加速度、背屈和跖屈的运动范围(ROM)以及初始接触、负荷反应、中间站立、终末站立、预摆动和摆动阶段的内翻-外翻。
在 CAI 患者中,受伤和未受伤的踝关节在角度-足角度、内翻-外翻 ROM、中间站立时的背屈、初始接触和终末站立时的内翻-外翻以及预摆动和摆动阶段(p<0.01)方面存在显著差异。与对照组的左、右踝关节相比,患者未受伤的踝关节的踝足速度(p=0.01)和加速度(p=0.01)均较低。此外,与对照组相比,患者未受伤的踝关节在初始接触、负荷反应、中间站立、终末站立、预摆动和摆动阶段时,背屈减少,内翻增加(p<0.017)。
这些结果表明,单侧 CAI 可能会影响对侧未受伤踝关节的步态生物力学。如果不及时治疗单侧 CAI,可能会导致对侧未受伤侧的发病率增加。当单侧 CAI 不适合手术治疗时,康复方案应同时针对双侧。