Department of Cardiology and Angiology II (Campus Bad Krozingen), Heart Center, University Hospital Freiburg, Südring 15, 79189 Bad Krozingen, Germany.
Europace. 2023 Feb 8;25(1):65-73. doi: 10.1093/europace/euac111.
The cornerstone of pulmonary vein (PV) isolation (PVI) is a wide-area circumferential ablation (WACA) resulting in an antral PVI area. Pulsed-field ablation (PFA) is a new nonthermal 'single-shot' PVI technique resulting in well-characterized posterior isolation areas. However, information on circumferential PVI area is lacking. Thus, we sought to characterize the circumferential antral PVI areas after PFA-PVI.
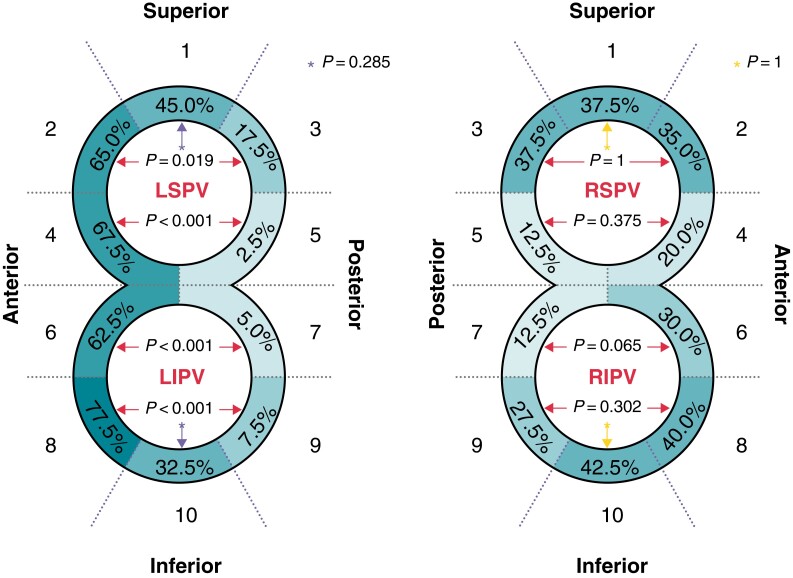
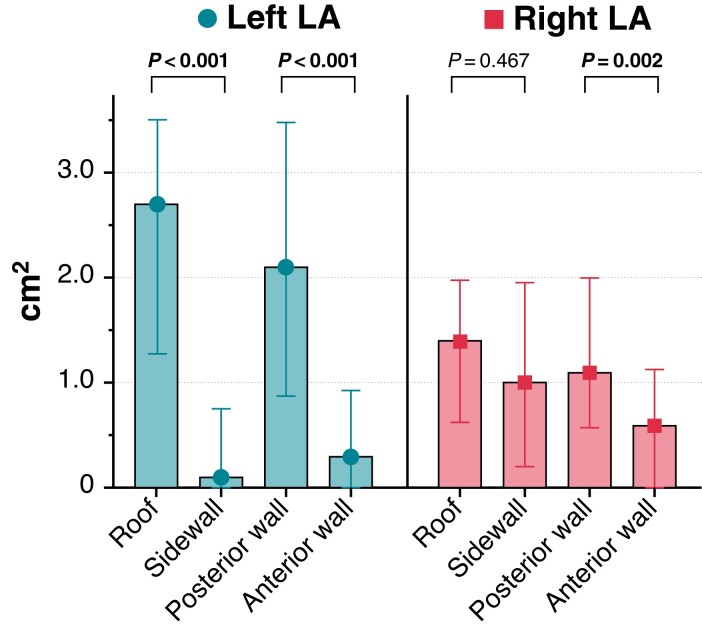
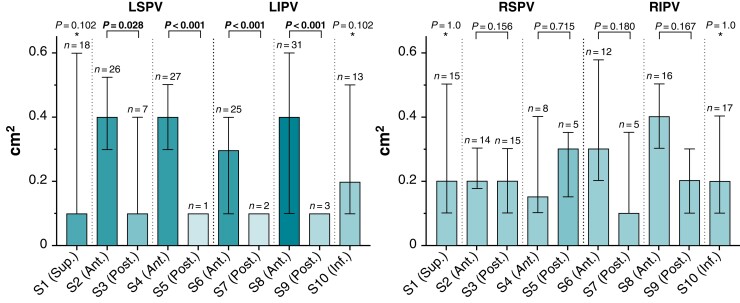
Atrial fibrillation (AF) patients underwent fluoroscopy-guided PVI with a pentaspline PFA catheter. Ultra-high-density voltage maps using a 20-polar circular mapping catheter were created before and immediately after PVI to identify and quantify (i) insufficient isolation areas per antral PV segment (10-segment model) and (ii) enlarged left atrial (LA) isolation areas (beyond the antral PV segments) per LA region (8-region model). The PFA-PVI with pre- (5469 ± 1822 points) and post-mapping (6809 ± 2769 points) was performed in 40 consecutive patients [age 62 ± 6 years, 25/40 (62.5%) paroxysmal AF]. Insufficient isolation areas were located most frequently in the anterior antral PV segments of the left PVs (62.5-77.5% of patients) with the largest extent (median ≥0.4 cm2) located in the same segments (segments 2/5/8). Enlarged LA isolation areas were located most frequently and most extensively on the posterior wall and roof region (89.5-100% of patients; median 1.1-2.7 cm2 per region).
Fluoroscopy-guided PFA-PVI frequently results in insufficient isolation areas in the left anterior antral PV segments and enlarged LA isolation areas on the posterior wall/roof, which both may be extensive. To optimize the procedure, full integration of PFA catheter visualization into three-dimensional-mapping systems is needed.
肺静脉(PV)隔离(PVI)的基石是广泛的环形消融(WACA),导致PV 口部消融面积。脉冲场消融(PFA)是一种新的非热“单次”PVI 技术,可导致特征性的后部隔离区域。然而,关于环形 PV 口部消融面积的信息尚缺乏。因此,我们试图描述 PFA-PVI 后的环形 PV 口部消融面积。
心房颤动(AF)患者在透视引导下行 PVI 治疗,使用五边形 PFA 消融导管。在 PVI 前后使用 20 极圆形标测导管创建超高密度电压图,以识别和量化(i)每个 PV 口部节段的不完全隔离区域(10 节段模型)和(ii)每个左心房(LA)区域的扩大的 LA 隔离区域(超出 PV 口部节段)(8 节段模型)。在 40 例连续患者中进行了 PFA-PVI(5469±1822 个点,术前;6809±2769 个点,术后)[年龄 62±6 岁,25/40(62.5%)阵发性 AF]。不完全隔离区域最常位于左 PV 口部的前侧(62.5%-77.5%的患者),最大范围(中位数≥0.4cm2)位于同一节段(节段 2/5/8)。扩大的 LA 隔离区域最常位于后侧壁和房顶区域,范围最广(89.5%-100%的患者;中位数每个区域 1.1-2.7cm2)。
透视引导下的 PFA-PVI 常导致左前侧 PV 口部的不完全隔离区域和后侧壁/房顶的扩大的 LA 隔离区域,两者都可能很广泛。为了优化该程序,需要将 PFA 导管可视化完全整合到三维标测系统中。