Universidade de São Paulo, Faculdade de Medicina, Instituto de Medicina Tropical de São Paulo, São Paulo, São Paulo, Brazil.
Faculdade Israelita de Ciências da Saúde Albert Einstein, São Paulo, São Paulo, Brazil.
Rev Inst Med Trop Sao Paulo. 2022 Jul 13;64:e49. doi: 10.1590/S1678-9946202264049. eCollection 2022.
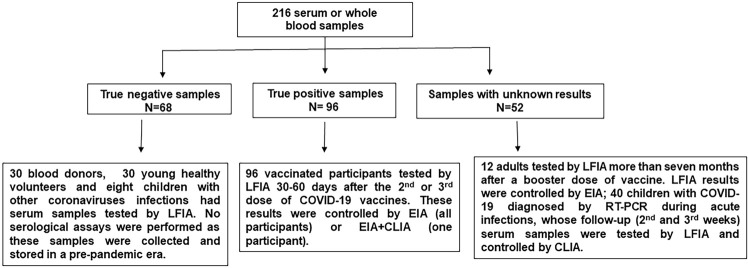
This study assessed the technical performance of a rapid lateral flow immunochromatographic assay (LFIA) for the detection of anti-SARS-CoV-2 IgG and compared LFIA results with chemiluminescent immunoassay (CLIA) results and an in-house enzyme immunoassay (EIA). To this end, a total of 216 whole blood or serum samples from three groups were analyzed: the first group was composed of 68 true negative cases corresponding to blood bank donors, healthy young volunteers, and eight pediatric patients diagnosed with other coronavirus infections. The serum samples from these participants were obtained and stored in a pre-COVID-19 period, thus they were not expected to have COVID-19. In the second group of true positive cases, we chose to replace natural cases of COVID-19 by 96 participants who were expected to have produced anti-SARS-CoV-2 IgG antibodies 30-60 days after the vaccine booster dose. The serum samples were collected on the same day that LFIA were tested either by EIA or CLIA. The third study group was composed of 52 participants (12 adults and 40 children) who did or did not have anti-SARS-CoV-2 IgG antibodies due to specific clinical scenarios. The 12 adults had been vaccinated more than seven months before LFIA testing, and the 40 children had non-severe COVID-19 diagnosed using RT-PCR during the acute phase of infection. They were referred for outpatient follow-up and during this period the serum samples were collected and tested by CLIA and LFIA. All tests were performed by the same healthcare operator and there was no variation of LFIA results when tests were performed on finger prick whole blood or serum samples, so that results were grouped for analysis. LFIA's sensitivity in detecting anti-SARS-CoV-2 IgG antibodies was 90%, specificity 97.6%, efficiency 93%, PPV 98.3%, NPV 86.6%, and likelihood ratio for a positive or a negative result were 37.5 and 0.01 respectively. There was a good agreement (Kappa index of 0.677) between LFIA results and serological (EIA or CLIA) results. In conclusion, LFIA analyzed in this study showed a good technical performance and agreement with reference serological assays (EIA or CLIA), therefore it can be recommended for use in the outpatient follow-up of non-severe cases of COVID-19 and to assess anti-SARS-CoV-2 IgG antibody production induced by vaccination and the antibodies decrease over time. However, LFIAs should be confirmed by using reference serological assays whenever possible.
本研究评估了一种用于检测抗 SARS-CoV-2 IgG 的快速侧向流动免疫层析测定法(LFIA)的技术性能,并将 LFIA 结果与化学发光免疫测定法(CLIA)结果和内部酶免疫测定法(EIA)进行了比较。为此,共分析了三组 216 份全血或血清样本:第一组由 68 例真阴性病例组成,对应于血库供者、健康年轻志愿者和 8 例诊断为其他冠状病毒感染的儿科患者。这些参与者的血清样本在 COVID-19 之前获得并储存,因此预计他们没有 COVID-19。在第二组真阳性病例中,我们选择用 96 名参与者替代 COVID-19 自然病例,这些参与者预计在疫苗加强剂量后 30-60 天会产生抗 SARS-CoV-2 IgG 抗体。血清样本是在同一天采集的,与 LFIA 一起通过 EIA 或 CLIA 进行检测。第三组由 52 名参与者(12 名成人和 40 名儿童)组成,这些参与者因特定的临床情况而具有或不具有抗 SARS-CoV-2 IgG 抗体。12 名成年人在 LFIA 检测前七个月以上接种了疫苗,40 名儿童在感染急性期通过 RT-PCR 诊断为非重症 COVID-19。他们被转介进行门诊随访,在此期间采集了血清样本并通过 CLIA 和 LFIA 进行了检测。所有测试均由同一位医疗保健操作员进行,当在指尖全血或血清样本上进行测试时,LFIA 结果没有变化,因此将结果分组进行分析。LFIA 检测抗 SARS-CoV-2 IgG 抗体的灵敏度为 90%,特异性为 97.6%,效率为 93%,PPV 为 98.3%,NPV 为 86.6%,阳性或阴性结果的似然比分别为 37.5 和 0.01。LFIA 结果与血清学(EIA 或 CLIA)结果之间存在良好的一致性(Kappa 指数为 0.677)。总之,本研究分析的 LFIA 显示出良好的技术性能和与参考血清学检测方法(EIA 或 CLIA)的一致性,因此可以推荐用于非重症 COVID-19 患者的门诊随访,以及评估疫苗诱导的抗 SARS-CoV-2 IgG 抗体产生及其随时间的减少。然而,只要有可能,LFIA 就应使用参考血清学检测方法进行确认。