Emergency Department and High Dependency Unit, San Luigi Gonzaga University Hospital, Orbassano (TO), Italy.
Department of Clinical and Biological Science, University of Turin, Regione Gonzole 10, Orbassano (TO), Italy.
BMC Public Health. 2022 Jan 7;22(1):45. doi: 10.1186/s12889-021-12409-w.
Patients that arrive in the emergency department (ED) with COVID-19-like syndromes testing negative at the first RT-PCR represent a clinical challenge because of the lack of evidence about their management available in the literature. Our first aim was to quantify the proportion of patients testing negative at the first RT-PCR performed in our Emergency Department (ED) that were confirmed as having COVID-19 at the end of hospitalization by clinical judgment or by any subsequent microbiological testing. Secondly, we wanted to identify which variables that were available in the first assessment (ED variables) would have been useful in predicting patients, who at the end of the hospital stay were confirmed as having COVID-19 (false-negative at the first RT-PCR).
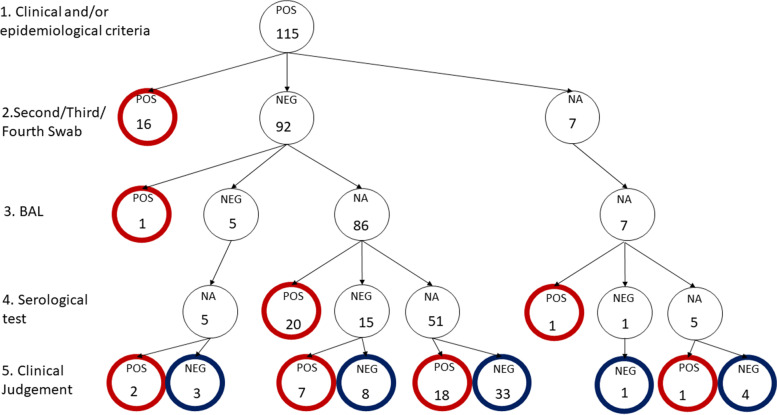
We retrospectively collected data of 115 negative patients from2020, March 1st to 2020, May 15th. Three experts revised patients' charts collecting information on the whole hospital stay and defining patients as COVID-19 or NOT-COVID-19. We compared ED variables in the two groups by univariate analysis and logistic regression.
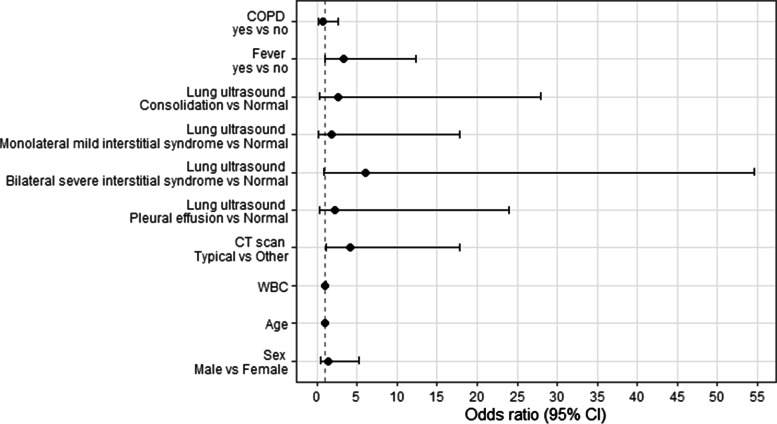
We classified 66 patients as COVID-19 and identified the other 49 as having a differential diagnosis (NOT-COVID), with a concordance between the three experts of 0.77 (95% confidence interval (95%CI) 0.66- 0.73). Only 15% of patients tested positive to a subsequent RT-PCR test, accounting for 25% of the clinically suspected. Having fever (odds ratio (OR) 3.32, (95%CI 0.97-12.31), p = 0.06), showing a typical pattern at the first lung ultrasound (OR 6.09, (95%CI 0.87-54.65), p = 0.08) or computed tomography scan (OR 4.18, (95%CI 1.11-17.86), p = 0.04) were associated with a higher probability of having COVID-19.
In patients admitted to ED with COVID-19 symptoms and negative RT-PCR a comprehensive clinical evaluation integrated with lung ultrasound and computed tomography could help to detect COVID-19 patients with a false negative RT-PCR result.
在急诊科(ED)出现 COVID-19 样综合征且首次 RT-PCR 检测为阴性的患者由于缺乏文献中关于其管理的证据而成为临床挑战。我们的第一个目标是量化在我们的急诊部(ED)首次进行 RT-PCR 检测为阴性的患者中,通过临床判断或任何后续微生物学检测最终被确诊为 COVID-19 的比例。其次,我们想确定在首次评估(ED 变量)中可用的哪些变量将有助于预测在住院期间最终被确诊为 COVID-19 的患者(首次 RT-PCR 检测为假阴性)。
我们回顾性收集了 2020 年 3 月 1 日至 2020 年 5 月 15 日期间 115 例阴性患者的数据。三位专家修订了患者的病历,收集了整个住院期间的信息,并将患者定义为 COVID-19 或非 COVID-19。我们通过单变量分析和逻辑回归比较了两组 ED 变量。
我们将 66 例患者归类为 COVID-19,并确定另外 49 例为其他诊断(非 COVID-19),三位专家之间的一致性为 0.77(95%置信区间(95%CI)为 0.66-0.73)。只有 15%的患者随后的 RT-PCR 检测呈阳性,占临床疑似病例的 25%。发热(优势比(OR)3.32,(95%CI 0.97-12.31),p=0.06)、首次肺部超声(OR 6.09,(95%CI 0.87-54.65),p=0.08)或计算机断层扫描(OR 4.18,(95%CI 1.11-17.86),p=0.04)呈现典型模式与 COVID-19 更高的可能性相关。
在因 COVID-19 症状且 RT-PCR 检测为阴性而入住 ED 的患者中,全面的临床评估结合肺部超声和计算机断层扫描可帮助检测到 RT-PCR 检测结果为假阴性的 COVID-19 患者。