Department of Internal Medicine, Seoul Medical Center, Seoul, Republic of Korea.
Division of Pulmonary and Critical Care Medicine, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea.
Thorac Cancer. 2022 Sep;13(17):2507-2514. doi: 10.1111/1759-7714.14587. Epub 2022 Jul 20.
Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) is used to evaluate hilar/interlobar/lobar lymph nodes. This study aimed to assess the clinical utility of EBUS-TBNA for station 10/11/12 lymph nodes (LNs) in patients with primary lung cancer.
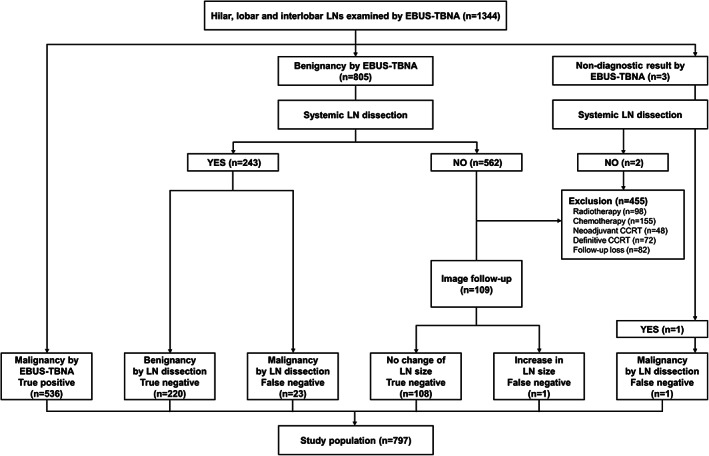
This was a retrospective analysis of a prospectively collected database of patients with primary lung cancer who underwent EBUS-TBNA for station 10/11/12 LNs from January 2015 to December 2019. Patients with benign results from EBUS-TBNA who did not undergo surgical sampling/clinical follow-up or who received radiotherapy/chemotherapy were excluded.
The analyses were conducted on 889 LNs from 797 patients. The overall diagnostic sensitivity, specificity, accuracy, negative predictive value (NPV), and positive predictive value of EBUS-TBNA were 95.7, 100, 97.3, 93.2, and 100%, respectively. Diagnostic sensitivity was significantly lower for LNs <10 mm than ≥10 mm in size (90.1% vs. 97.8%; p < 0.001). There was no significant difference in diagnostic performance according to the nodal station (10 vs. 11/12) and left- versus right-sided LNs. The diagnostic sensitivity (100 vs. 95.5%; p = 0.221) and specificity (100 vs. 100%) of N3 LNs was not significantly different from those of N1 LNs. In this study, eight (8/91, 8.8%) patients with cN1 NSCLC received neoadjuvant treatment based on the results of EBUS-TBNA.
EBUS-TBNA accurately evaluates station 10/11/12 LNs of both N1 and N3 disease. The diagnostic performances of EBUS-TBNA for station 10/11/12 LNs seem to be comparable to those of EBUS-TBNA for mediastinal LNs.
经支气管超声引导针吸活检术(EBUS-TBNA)用于评估肺门/叶间/肺段淋巴结。本研究旨在评估 EBUS-TBNA 对原发性肺癌患者第 10/11/12 站淋巴结(LNs)的临床应用价值。
这是一项对 2015 年 1 月至 2019 年 12 月期间接受 EBUS-TBNA 第 10/11/12 站 LN 活检的原发性肺癌患者前瞻性数据库的回顾性分析。EBUS-TBNA 结果为良性但未进行手术取样/临床随访或接受放疗/化疗的患者被排除在外。
共对 797 例患者的 889 个 LN 进行了分析。EBUS-TBNA 的总体诊断敏感性、特异性、准确性、阴性预测值(NPV)和阳性预测值分别为 95.7%、100%、97.3%、93.2%和 100%。大小<10mm 的 LN 的诊断敏感性明显低于≥10mm 的 LN(90.1%比 97.8%;p<0.001)。根据淋巴结站(第 10 站与 11/12 站)和左/右侧 LN,诊断性能无显著差异。N3 LNs 的诊断敏感性(100%比 95.5%;p=0.221)和特异性(100%比 100%)与 N1 LNs 无显著差异。在本研究中,8 例(8/91,8.8%)cN1 NSCLC 患者根据 EBUS-TBNA 结果接受了新辅助治疗。
EBUS-TBNA 可准确评估 N1 和 N3 疾病的第 10/11/12 站 LNs。EBUS-TBNA 对第 10/11/12 站 LNs 的诊断性能似乎与 EBUS-TBNA 对纵隔 LNs 的诊断性能相当。