Wills Nicola K, Nair Nikhil, Patel Kashyap, Sikder Omaike, Adriaanse Marguerite, Eikelboom John, Wasserman Sean
Department of Medicine, University of Cape Town, Cape Town, South Africa.
Michael G. DeGroote School of Medicine, McMaster University, Hamilton, Ontario, Canada.
Open Forum Infect Dis. 2022 Jun 7;9(7):ofac285. doi: 10.1093/ofid/ofac285. eCollection 2022 Jul.
Randomized controlled trials (RCTs) have reported inconsistent effects from intensified anticoagulation on clinical outcomes in coronavirus disease 2019 (COVID-19). We performed an aggregate data meta-analysis from available trials to quantify effect on nonfatal and fatal outcomes and identify subgroups who may benefit.
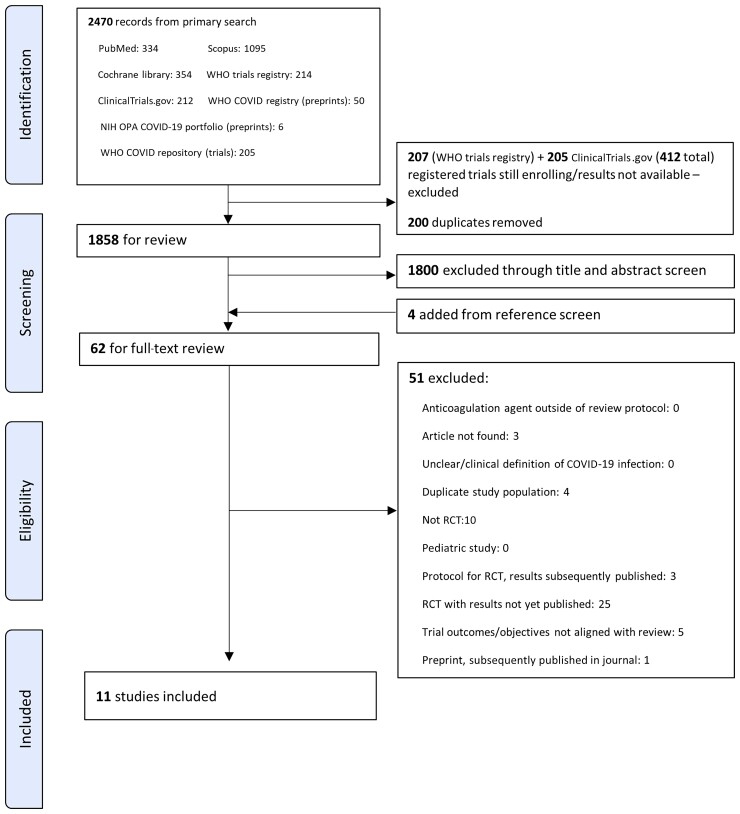
We searched multiple databases for RCTs comparing intensified (intermediate or therapeutic dose) vs prophylactic anticoagulation in adults with laboratory-confirmed COVID-19 through 19 January 2022. We used random-effects meta-analysis to estimate pooled risk ratios for mortality, thrombotic, and bleeding events (at end of follow-up or discharge) and performed subgroup analysis for clinical setting and dose of intensified anticoagulation.
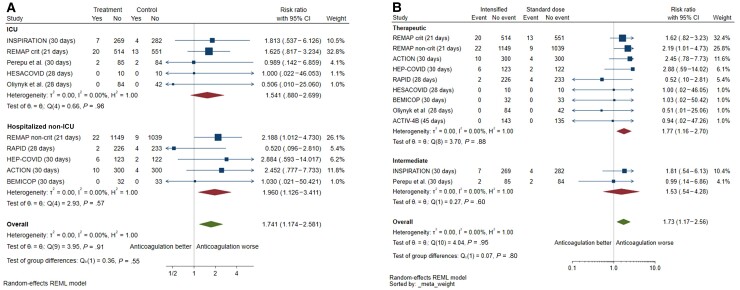
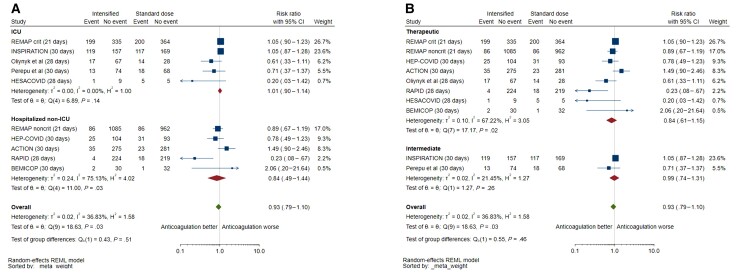
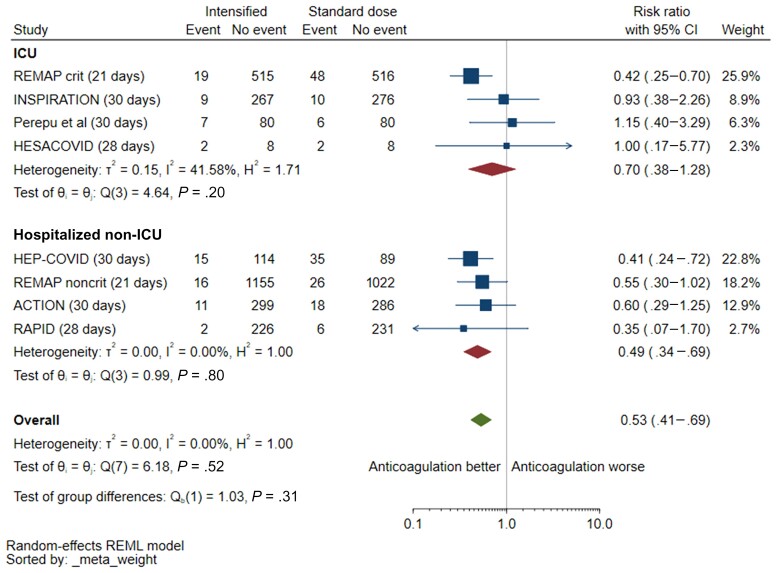
Eleven RCTs were included (N = 5873). Intensified vs prophylactic anticoagulation was not associated with a mortality reduction up to 45 days (risk ratio [RR], 0.93 [95% confidence interval {CI}, .79-1.10]). There was a possible signal of mortality reduction for non-intensive care unit (ICU) patients, although with low precision and high heterogeneity (5 studies; RR, 0.84 [95% CI, .49-1.44]; = 75%). Risk of venous thromboembolism was reduced (RR, 0.53 [95% CI, .41-.69]; = 0%), with effect driven by therapeutic rather than intermediate dosing (interaction = .04). Major bleeding was increased with intensified anticoagulation (RR, 1.73 [95% CI, 1.17-2.56]) with no interaction for dosing and clinical setting.
Intensified anticoagulation has no effect on mortality among hospitalized adults with COVID-19 and is associated with increased bleeding risk. The observed reduction in venous thromboembolism risk and trend toward reduced mortality in non-ICU settings requires exploration in additional RCTs. CRD42021273449 (PROSPERO).
随机对照试验(RCT)报告了强化抗凝治疗对2019冠状病毒病(COVID-19)临床结局的影响并不一致。我们对现有试验进行汇总数据荟萃分析,以量化对非致命和致命结局的影响,并确定可能受益的亚组。
我们检索了多个数据库,以查找截至2022年1月19日比较强化(中等剂量或治疗剂量)与预防性抗凝治疗对实验室确诊的成人COVID-19患者影响的随机对照试验。我们使用随机效应荟萃分析来估计死亡率、血栓形成和出血事件(随访结束或出院时)的合并风险比,并对强化抗凝治疗的临床环境和剂量进行亚组分析。
纳入了11项随机对照试验(N = 5873)。强化抗凝与预防性抗凝相比,在45天内并未降低死亡率(风险比[RR],0.93[95%置信区间{CI},0.79 - 1.10])。对于非重症监护病房(ICU)患者,有降低死亡率的可能信号,尽管精度较低且异质性较高(5项研究;RR,0.84[95%CI,0.49 - 1.44];I² = 75%)。静脉血栓栓塞风险降低(RR,0.53[95%CI,0.41 - 0.69];I² = 0%),其效果由治疗剂量而非中等剂量驱动(交互作用P = 0.04)。强化抗凝治疗会增加大出血风险(RR,1.73[95%CI,1.17 - 2.56]),剂量和临床环境之间无交互作用。
强化抗凝治疗对住院COVID-19成人患者的死亡率无影响,且与出血风险增加相关。在非ICU环境中观察到的静脉血栓栓塞风险降低以及死亡率降低的趋势,需要在更多随机对照试验中进行探索。CRD42021273449(PROSPERO)