Department of Oncology and Pathology, Karolinska Institutet, Stockholm, Sweden.
Department of Laboratory Medicine, University of California San Francisco, San Francisco, CA.
J Clin Oncol. 2022 Dec 10;40(35):4071-4082. doi: 10.1200/JCO.21.02844. Epub 2022 Jul 21.
To assess the long-term (20-year) endocrine therapy benefit in premenopausal patients with breast cancer.
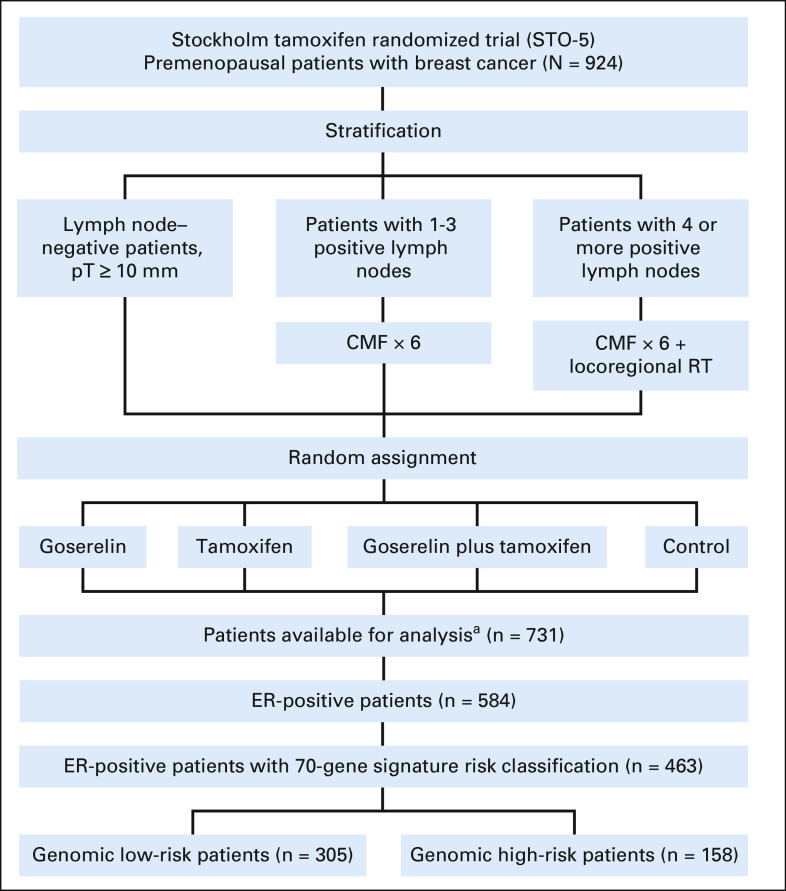
Secondary analysis of the Stockholm trial (STO-5, 1990-1997) randomly assigning 924 premenopausal patients to 2 years of goserelin (3.6 mg subcutaneously once every 28 days), tamoxifen (40 mg orally once daily), combined goserelin and tamoxifen, or no adjuvant endocrine therapy (control) is performed. Random assignment was stratified by lymph node status; lymph node-positive patients (n = 459) were allocated to standard chemotherapy (cyclophosphamide, methotrexate, and fluorouracil). Primary tumor immunohistochemistry (n = 731) and gene expression profiling (n = 586) were conducted in 2020. The 70-gene signature identified genomic low-risk and high-risk patients. Kaplan-Meier analysis, multivariable Cox proportional hazard regression, and multivariable time-varying flexible parametric modeling assessed the long-term distant recurrence-free interval (DRFI). Swedish high-quality registries allowed a complete follow-up of 20 years.
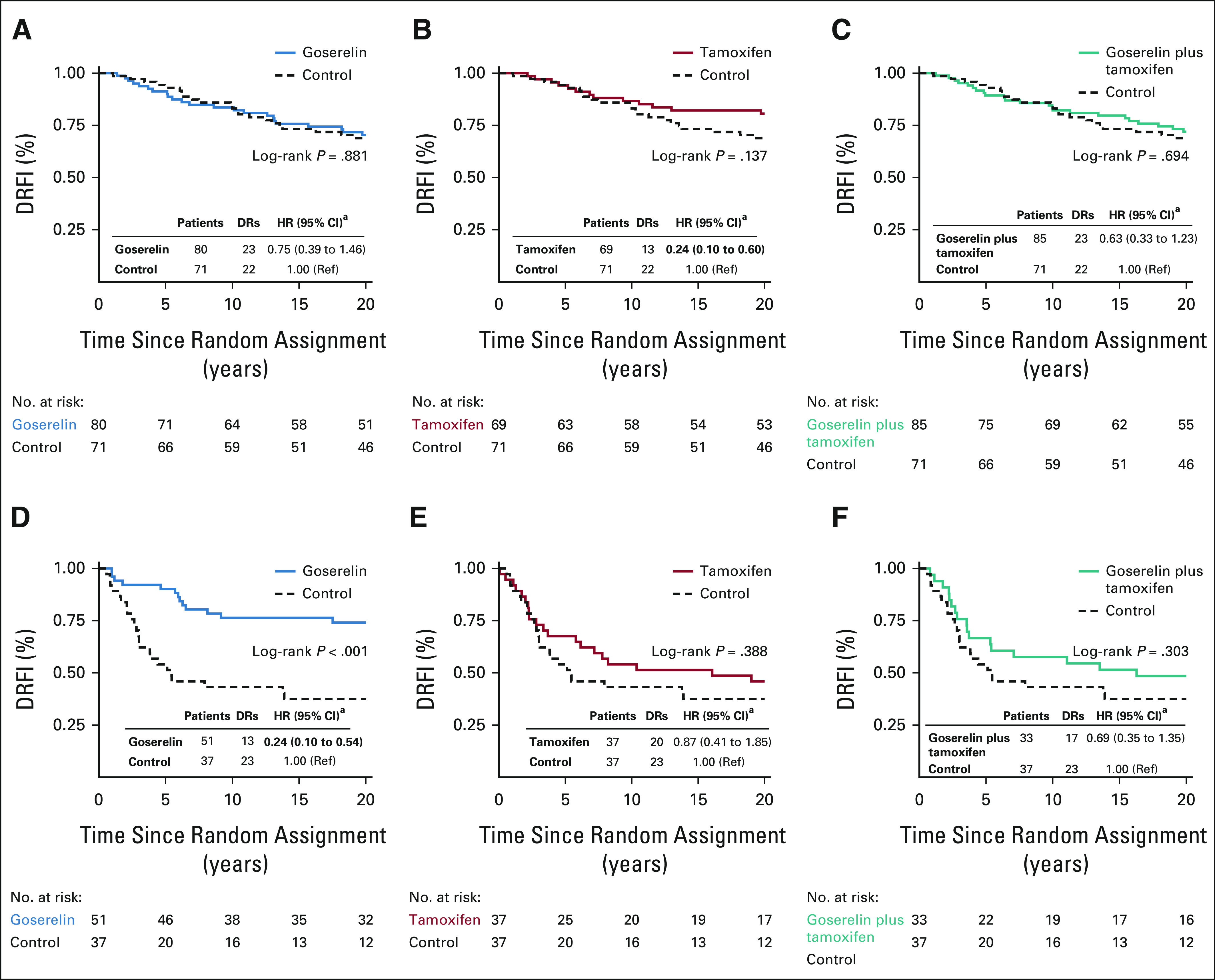
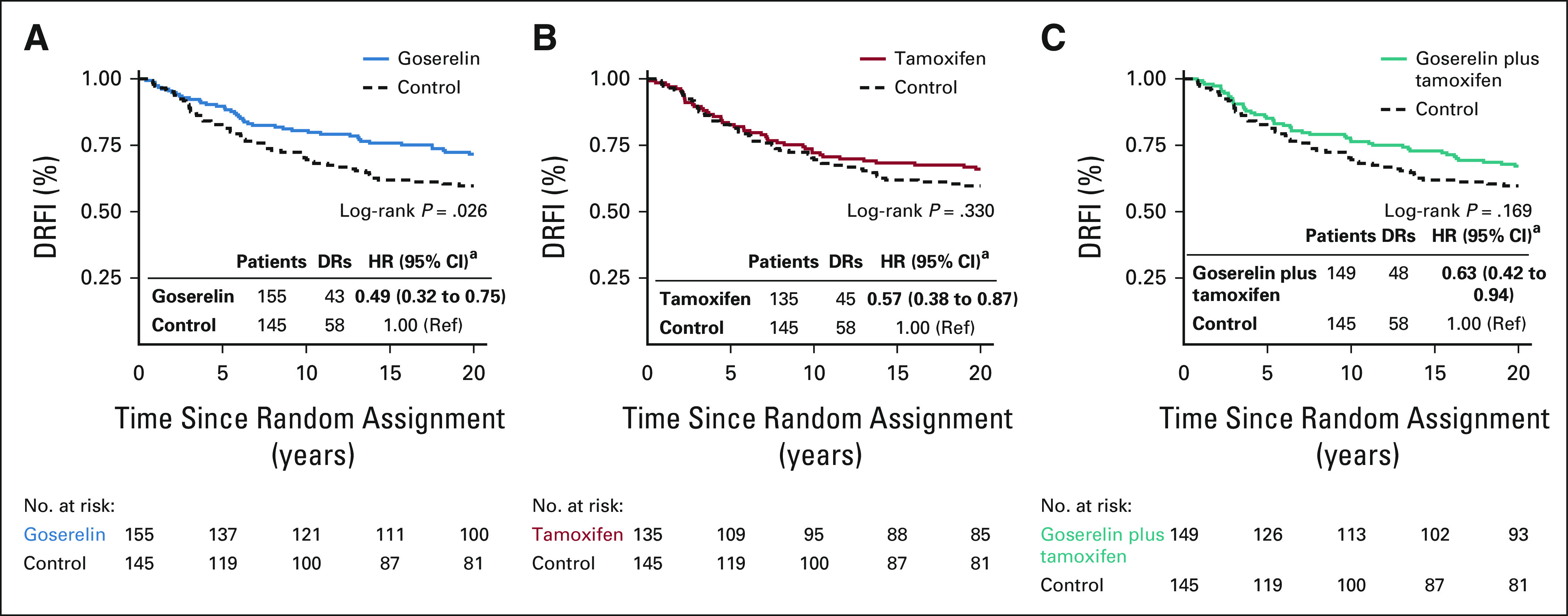
In estrogen receptor-positive patients (n = 584, median age 47 years), goserelin, tamoxifen, and the combination significantly improved long-term distant recurrence-free interval compared with control (multivariable hazard ratio [HR], 0.49; 95% CI, 0.32 to 0.75, HR, 0.57; 95% CI, 0.38 to 0.87, and HR, 0.63; 95% CI, 0.42 to 0.94, respectively). Significant goserelin-tamoxifen interaction was observed ( = .016). Genomic low-risk patients (n = 305) significantly benefitted from tamoxifen (HR, 0.24; 95% CI, 0.10 to 0.60), and genomic high-risk patients (n = 158) from goserelin (HR, 0.24; 95% CI, 0.10 to 0.54). Increased risk from the addition of tamoxifen to goserelin was seen in genomic high-risk patients (HR, 3.36; 95% CI, 1.39 to 8.07). Moreover, long-lasting 20-year tamoxifen benefit was seen in genomic low-risk patients, whereas genomic high-risk patients had early goserelin benefit.
This study shows 20-year benefit from 2 years of adjuvant endocrine therapy in estrogen receptor-positive premenopausal patients and suggests differential treatment benefit on the basis of tumor genomic characteristics. Combined goserelin and tamoxifen therapy showed no benefit over single treatment. Long-term follow-up to assess treatment benefit is critical.
评估绝经前乳腺癌患者长期(20 年)内分泌治疗的获益。
对斯德哥尔摩试验(STO-5,1990-1997 年)进行二次分析,该试验随机分配 924 例绝经前患者接受 2 年戈舍瑞林(3.6mg 皮下注射,每 28 天一次)、他莫昔芬(40mg 口服,每日一次)、戈舍瑞林联合他莫昔芬或无辅助内分泌治疗(对照组)。随机分配按淋巴结状态分层;淋巴结阳性患者(n=459)接受标准化疗(环磷酰胺、甲氨蝶呤和氟尿嘧啶)。2020 年进行了原发性肿瘤免疫组织化学(n=731)和基因表达谱分析(n=586)。70 基因特征确定了基因组低风险和高风险患者。Kaplan-Meier 分析、多变量 Cox 比例风险回归和多变量时变灵活参数建模评估了长期远处无复发生存期(DRFI)。瑞典高质量的登记册允许对 20 年的完整随访。
在雌激素受体阳性患者(n=584,中位年龄 47 岁)中,与对照组相比,戈舍瑞林、他莫昔芬和联合治疗显著改善了长期远处无复发生存期(多变量危险比[HR],0.49;95%CI,0.32 至 0.75;HR,0.57;95%CI,0.38 至 0.87;HR,0.63;95%CI,0.42 至 0.94)。观察到戈舍瑞林-他莫昔芬有显著的相互作用(=0.016)。基因组低风险患者(n=305)从他莫昔芬中显著获益(HR,0.24;95%CI,0.10 至 0.60),而基因组高风险患者(n=158)从戈舍瑞林中获益(HR,0.24;95%CI,0.10 至 0.54)。在基因组高风险患者中,添加他莫昔芬至戈舍瑞林的风险增加(HR,3.36;95%CI,1.39 至 8.07)。此外,在基因组低风险患者中观察到长达 20 年的他莫昔芬获益,而基因组高风险患者则早期获益于戈舍瑞林。
本研究显示,雌激素受体阳性绝经前患者接受 2 年辅助内分泌治疗可获得 20 年获益,并提示基于肿瘤基因组特征存在不同的治疗获益。戈舍瑞林联合他莫昔芬治疗与单一治疗相比无获益。进行长期随访以评估治疗获益至关重要。