Center for Personalized Cancer Therapy and Division of Hematology and Oncology, Department of Medicine, UC San Diego Moores Cancer Center, La Jolla, CA, USA.
Department of Oncology, The Sidney Kimmel Comprehensive Cancer Center, The Johns Hopkins Hospital, Baltimore, MD, USA.
Mol Oncol. 2024 Apr;18(4):956-968. doi: 10.1002/1878-0261.13293. Epub 2023 Nov 16.
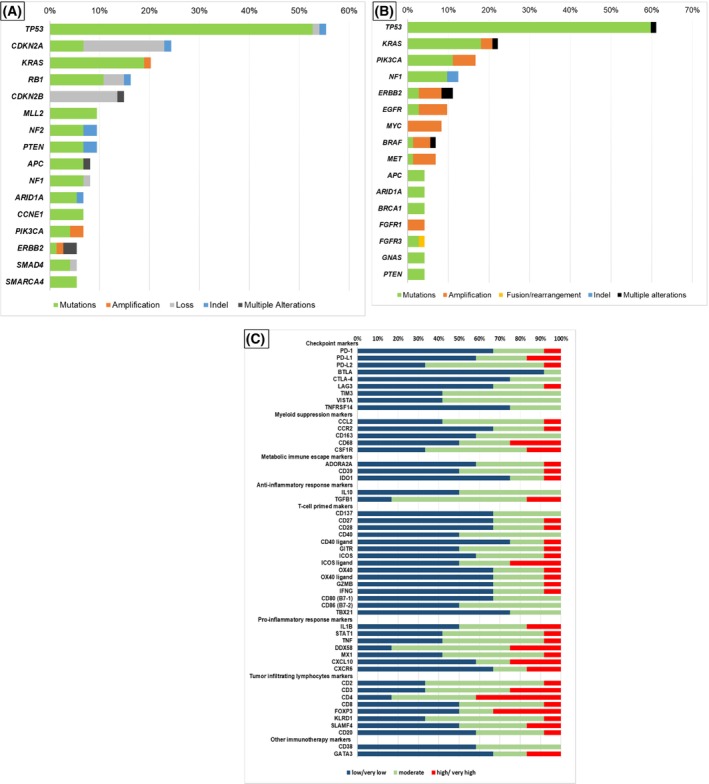
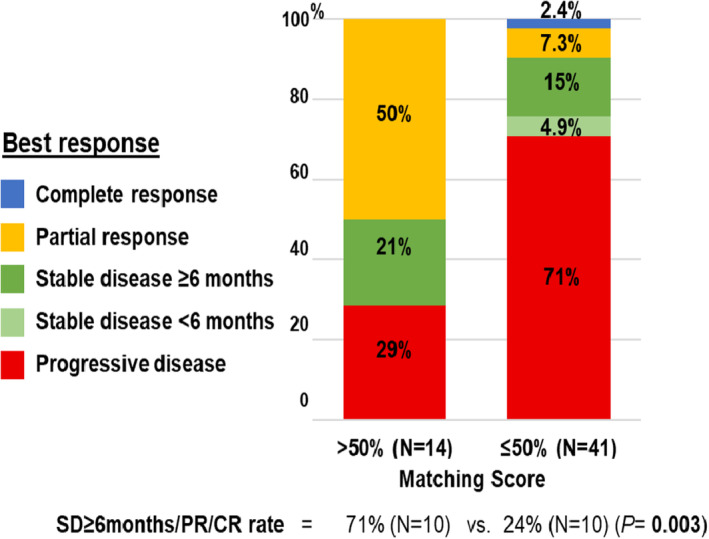
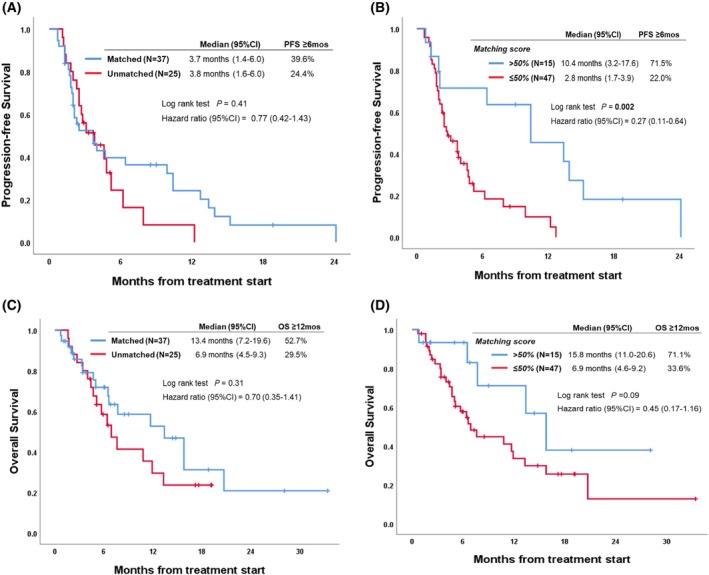
Carcinoma of unknown primary (CUP) is a difficult-to-manage malignancy. Multi-omic profiles and treatment outcome vs. degree of precision matching were assessed. Tumours underwent next-generation sequencing (NGS) [tissue and/or blood-derived cell-free DNA (cfDNA)]. Selected patients had transcriptome-based immune profiling and/or programmed cell death 1 ligand 1 (PD-L1) immunohistochemistry analysis. Patients could be reviewed by a Molecular Tumor Board, but physicians chose the therapy. Of 6497 patients in the precision database, 97 had CUP. The median number of pathogenic tissue genomic alterations was 4 (range, 0-25), and for cfDNA, was 2 (range, 0-9). Each patient had a distinct molecular landscape. Food and Drug Administration (FDA)-approved biomarkers included the following: PD-L1 ≥ 1%, 30.9% of CUPs tested; microsatellite instability, 3.6%; tumour mutational burden ≥ 10 mutations·Mb, 23%; and neurotrophic receptor tyrosine kinase (NTRK) fusions, 0%. RNA-based immunograms showed theoretically druggable targets: lymphocyte activation gene 3 protein (LAG-3), macrophage colony-stimulating factor 1 receptor (CSF1R), adenosine receptor A2 (ADORA2) and indoleamine 2,3-dioxygenase 1 (IDO1). Overall, 56% of patients had ≥ 1 actionable biomarker (OncoKB database). To quantify the degree of matching (tumours to drugs), a Matching Score (MS; roughly equivalent to number of alterations targeted/total number of deleterious alterations) was calculated post hoc. Comparing evaluable treated patients [MS high, > 50% (N = 15) vs. low ≤ 50% (N = 47)], median progression-free survival was 10.4 vs. 2.8 months (95% CI 0.11-0.64; HR 0.27; P = 0.002); survival, 15.8 vs. 6.9 months (95% CI 0.17-1.16; HR 0.45; P = 0.09); and clinical benefit rate (stable disease ≥ 6 months/partial/complete response), 71% vs. 24% (P = 0.003). Higher MS was the only factor that predicted improvement in outcome variables after multivariate analysis. In conclusion, CUPs are molecularly complex. Treatments with high degrees of matching to molecular alterations (generally achieved by individualized combinations) correlated with improved outcomes.
原发灶不明癌(CUP)是一种难以治疗的恶性肿瘤。评估了多组学特征和治疗结果与精准匹配程度的关系。肿瘤进行了下一代测序(NGS)[组织和/或血液衍生的游离 DNA(cfDNA)]。选择部分患者进行基于转录组的免疫分析和/或程序性死亡配体 1(PD-L1)免疫组化分析。患者可由分子肿瘤委员会进行评估,但医生选择治疗方法。在精准数据库中的 6497 名患者中,有 97 名患有 CUP。组织基因组改变的中位数量为 4(范围,0-25),cfDNA 为 2(范围,0-9)。每个患者都有独特的分子景观。食品和药物管理局(FDA)批准的生物标志物包括以下内容:PD-L1≥1%,97%的 CUP 测试;微卫星不稳定性,3.6%;肿瘤突变负担≥10 个突变·Mb,23%;和神经生长因子受体酪氨酸激酶(NTRK)融合,0%。基于 RNA 的免疫组显示了理论上可药物治疗的靶点:淋巴细胞激活基因 3 蛋白(LAG-3)、巨噬细胞集落刺激因子 1 受体(CSF1R)、腺苷受体 A2(ADORA2)和吲哚胺 2,3-双加氧酶 1(IDO1)。总体而言,56%的患者具有≥1 个可操作的生物标志物(OncoKB 数据库)。为了量化匹配程度(肿瘤与药物),在事后计算了匹配评分(MS;大致相当于靶向的改变数量/总有害改变数量)。比较可评估的治疗患者[MS 高,>50%(N=15)与低≤50%(N=47)],中位无进展生存期为 10.4 与 2.8 个月(95%CI 0.11-0.64;HR 0.27;P=0.002);生存时间为 15.8 与 6.9 个月(95%CI 0.17-1.16;HR 0.45;P=0.09);临床获益率(稳定疾病≥6 个月/部分/完全缓解)为 71%与 24%(P=0.003)。多变量分析后,只有较高的 MS 是预测生存结果改善的唯一因素。总之,CUP 具有复杂的分子特征。与分子改变高度匹配的治疗方法(通常通过个体化组合实现)与改善的结果相关。