Aberdeen Centre for Health Data Science, University of Aberdeen, Aberdeen, UK.
NHS Grampian, Aberdeen, UK.
Nephrol Dial Transplant. 2023 May 4;38(5):1170-1182. doi: 10.1093/ndt/gfac224.
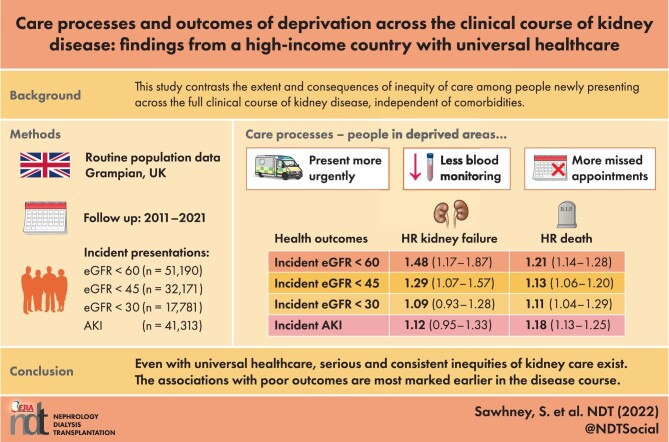
No single study contrasts the extent and consequences of inequity of kidney care across the clinical course of kidney disease.
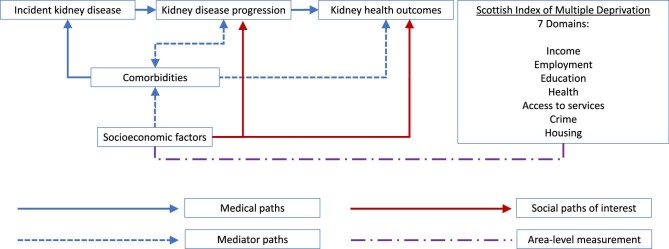
This population study of Grampian (UK) followed incident presentations of acute kidney injury (AKI) and incident estimated glomerular filtration rate (eGFR) thresholds of <60, <45 and <30 mL/min/1.73 m2 in separate cohorts (2011-2021). The key exposure was area-level deprivation (lowest quintile of the Scottish Index of Multiple Deprivation). Outcomes were care processes (monitoring, prescribing, appointments, unscheduled care), long-term mortality and kidney failure. Modelling involved multivariable logistic regression, negative binomial regression and cause-specific Cox models with and without adjustment of comorbidities.
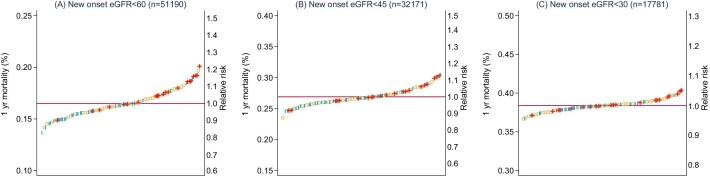
There were 41 313, 51 190, 32 171 and 17 781 new presentations of AKI and eGFR thresholds <60, <45 and <30 mL/min/1.73 m2. A total of 6.1-7.8% of the population was from deprived areas and (versus all others) presented on average 5 years younger, with more diabetes and pulmonary and liver disease. Those from deprived areas were more likely to present initially in hospital, less likely to receive community monitoring, less likely to attend appointments and more likely to have an unplanned emergency department or hospital admission episode. Deprivation had the greatest association with long-term kidney failure at the eGFR <60 mL/min/1.73 m2 threshold {adjusted hazard ratio [HR] 1.48 [95% confidence interval (CI) 1.17-1.87]} and this association decreased with advancing disease severity [HR 1.09 (95% CI 0.93-1.28) at eGFR <30 mL/min/1.73 m2), with a similar pattern for mortality. Across all analyses the most detrimental associations of deprivation were an eGFR threshold <60 mL/min/1.73 m2, AKI, males and those <65 years of age.
Even in a high-income country with universal healthcare, serious and consistent inequities in kidney care exist. The poorer care and outcomes with area-level deprivation were greater earlier in the disease course.
目前尚无研究对比肾脏病临床病程中肾脏护理的公平性程度和结果。
本项以英国 Grampian 人群为基础的研究纳入了急性肾损伤(AKI)和肾小球滤过率(eGFR)<60、<45 和 <30ml/min/1.73m2 的多个队列,分别分析了不同队列中人群的发病情况。主要暴露因素为地区水平的贫困(苏格兰多重贫困指数最低五分位数)。研究结局为护理过程(监测、处方、预约、非计划性医疗)、长期死亡率和肾衰竭。采用多变量逻辑回归、负二项回归和有及无合并症调整的特定原因 Cox 模型进行建模。
AKI 和 eGFR <60、<45 和 <30ml/min/1.73m2 的新发病例分别为 41313、51190、32171 和 17781 例。共有 6.1%-7.8%的人群来自贫困地区,与其他人群相比,平均发病年龄低 5 岁,合并糖尿病、肺部和肝脏疾病的比例更高。来自贫困地区的患者初次发病时更有可能住院,社区监测的可能性更小,预约就诊的可能性更小,无计划的急诊科或住院治疗的可能性更大。在 eGFR <60ml/min/1.73m2 这一阈值,与长期肾衰竭相关的贫困程度最大[调整后的危险比(HR)1.48(95%置信区间(CI)1.17-1.87)],随着疾病严重程度的进展,这种关联减弱[在 eGFR <30ml/min/1.73m2 时,HR 为 1.09(95%CI 0.93-1.28)],死亡率也呈现出类似的模式。在所有分析中,与贫困相关的最不利因素是 eGFR <60ml/min/1.73m2、AKI、男性和<65 岁的患者。
即使在一个全民医疗保健的高收入国家,肾脏护理也存在严重且持续的不公平现象。在疾病早期,与地区贫困相关的护理质量更差,结局更差。