Department of Cardiology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, P. R. China.
Clin Cardiol. 2022 Sep;45(9):928-935. doi: 10.1002/clc.23880. Epub 2022 Jul 23.
Initiating ivabradine in acute heart failure (HF) is still controversial.
Ivabradine might be effective to be added in acute but hemodynamically stable HF.
A retrospective cohort of hemodynamically stable acute HF patients was enrolled from January 2018 to January 2020 and followed until July 2020. The primary endpoints were all-cause mortality and rehospitalization for HF. Secondary endpoints included heart rate (HR), cardiac function measured by New York Heart Association (NYHA) class, and left ventricular ejection fraction (LVEF) and adverse events, which were compared between patients with or without ivabradine.
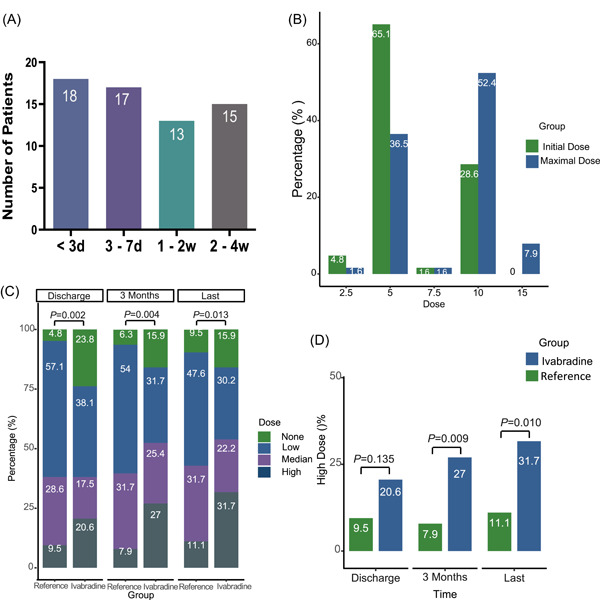
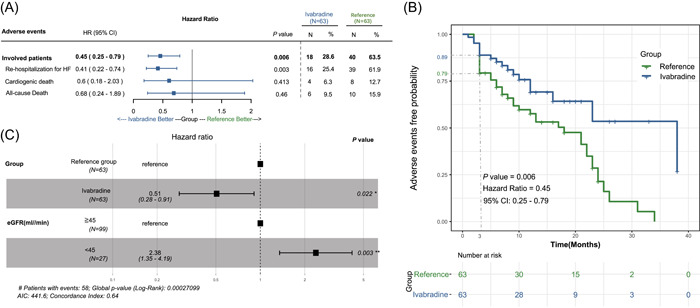
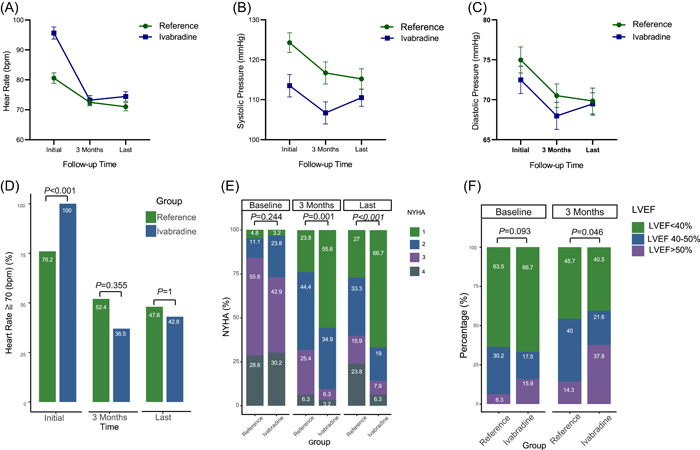
A total of 126 patients were enrolled (50 males, median age 54 years, 81% with decompensated HF, median follow-up of 9 months). In patients treated with ivabradine, although baseline HRs were higher than the reference group (96 vs. 80 bpm), they were comparable after 3 months; more patients tolerated high doses of β-blockers (27% vs. 7.9%), improved to NYHA class I function (55.6% vs. 23.8%) and exhibited normal LVEFs (37.8% vs. 14.3%) than the reference group (all p < .05). Ivabradine was associated with a significant reduction of rehospitalization for HF than the reference group (25.4% vs.61.9%), with longer event-free survival times (hazard ratio: 0.45, 95% confidence interval [CI]: 0.25-0.79), and was related with primary endpoints negatively (hazard ratio 0.51, 95% CI: 0.28-0.91) (all p < .05).
In patients with acute but hemodynamically stable HF, ivabradine may significantly reduce HR, improve cardiac function, and reduce HF rehospitalization.
在急性心力衰竭(HF)中起始使用伊伐布雷定仍存在争议。
伊伐布雷定可能对急性但血流动力学稳定的 HF 有益。
本研究回顾性纳入了 2018 年 1 月至 2020 年 1 月间血流动力学稳定的急性 HF 患者,并随访至 2020 年 7 月。主要终点为全因死亡率和因 HF 再住院。次要终点包括心率(HR)、纽约心脏协会(NYHA)分级评估的心脏功能以及左心室射血分数(LVEF)和不良事件,并比较了使用伊伐布雷定与未使用伊伐布雷定患者之间的差异。
共纳入 126 例患者(男性 50 例,中位年龄 54 岁,81%为失代偿性 HF,中位随访 9 个月)。在使用伊伐布雷定的患者中,尽管基线 HR 高于对照组(96 比 80 bpm),但在 3 个月后无差异;更多患者能够耐受高剂量β受体阻滞剂(27%比 7.9%),NYHA 心功能分级改善至 I 级(55.6%比 23.8%),LVEF 恢复正常(37.8%比 14.3%)的比例高于对照组(均 P<.05)。与对照组相比,伊伐布雷定组 HF 再住院率显著降低(25.4%比 61.9%),无事件生存时间更长(风险比:0.45,95%置信区间[CI]:0.25-0.79),且与主要终点呈负相关(风险比 0.51,95% CI:0.28-0.91)(均 P<.05)。
在急性但血流动力学稳定的 HF 患者中,伊伐布雷定可显著降低 HR、改善心功能并降低 HF 再住院率。