Department of Health Economics and Health Services Research, University Medical Center Hamburg-Eppendorf, Martinistr. 52, 20246, Hamburg, Germany.
Institute of Epidemiology and Medical Biometry, Ulm University, Ulm, Germany.
J Gen Intern Med. 2023 Feb;38(3):641-647. doi: 10.1007/s11606-022-07691-2. Epub 2022 Jul 25.
Fragility fractures are one of the leading causes of disability in older adults. Yet, evidence for effectiveness and cost-effectiveness of preventive approaches combining bone health and fall prevention is rare.
To conduct a health-economic evaluation of the German osteoporotic fracture prevention program in rural areas (OFRA).
Secondary cluster-randomized intervention study based on routine data.
All districts in five federal states in Germany were cluster-randomized as intervention or control districts. OFRA was offered to community-living (a) women aged 75-79 years or (b) women and men aged 70-84 years with a prior fragility fracture in the intervention districts. Individuals who meet these criteria in the control districts were assigned to the control group.
OFRA comprised mobility and falls prevention classes, examination of bone health by bone density measurement, and consultation on safety in the home living environment.
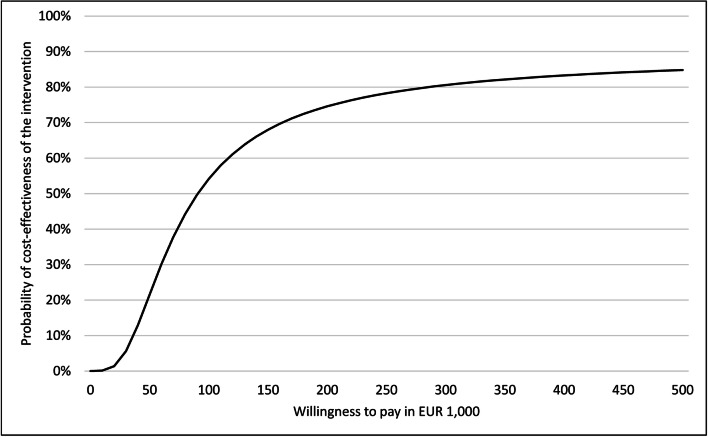
We measured health-care costs and effectiveness in terms of time to fragility fracture or death within 1 year after initial contact, based on health insurance claims data. Implementation costs were recorded by the intervention performers. We calculated an incremental cost-effectiveness ratio (ICER) and employed the net-benefit approach to construct a cost-effectiveness acceptability curve (CEAC).
There were 9408 individuals in the intervention group and 27,318 in the control group. Mean time to fragility fracture or death (difference: 0.82 days) and health-care costs (difference: 111.73€, p < .01) were reduced, but mean intervention costs (difference: 260.10€) increased total costs (difference: 148.37€, p < .001) in the intervention group. The ICER per fracture-free year of survival was 66,094.63€. The CEAC showed no acceptable probability of cost-effectiveness at a reasonable willingness to pay.
OFRA showed reduced rates of fragility fractures, but had high implementation costs, resulting in an unfavorable ICER. The cost-effectiveness of OFRA may improve with a longer follow-up.
脆性骨折是导致老年人残疾的主要原因之一。然而,将骨骼健康和防跌倒措施结合起来的预防方法的有效性和成本效益证据很少。
对德国农村地区骨质疏松性骨折预防计划(OFRA)进行健康经济评估。
基于常规数据的二级聚类随机干预研究。
德国五个联邦州的所有地区均进行聚类随机分组,分为干预组或对照组。OFRA 提供给社区居住的(a)75-79 岁女性或(b)70-84 岁有脆性骨折既往史的女性和男性。在对照组中符合这些标准的个体被分配到对照组。
OFRA 包括运动和防跌倒课程、骨密度测量检查骨骼健康以及咨询家庭生活环境中的安全问题。
我们根据健康保险索赔数据,以初次接触后 1 年内发生脆性骨折或死亡的时间来衡量医疗保健成本和效果。干预执行者记录实施成本。我们计算了增量成本效益比(ICER),并采用净收益方法构建成本效益可接受性曲线(CEAC)。
干预组有 9408 人,对照组有 27318 人。脆性骨折或死亡的平均时间(差异:0.82 天)和医疗保健成本(差异:111.73 欧元,p <.01)降低,但干预组的平均干预成本(差异:260.10 欧元)增加了总费用(差异:148.37 欧元,p <.001)。无骨折生存的每 1 年的 ICER 为 66094.63 欧元。CEAC 显示,在合理的支付意愿下,没有成本效益的可接受概率。
OFRA 降低了脆性骨折的发生率,但实施成本较高,导致不利的 ICER。随着随访时间的延长,OFRA 的成本效益可能会提高。