Vychopen Martin, Hamed Motaz, Bahna Majd, Racz Attila, Ilic Inja, Salemdawod Abdallah, Schneider Matthias, Lehmann Felix, Eichhorn Lars, Bode Christian, Jacobs Andreas H, Behning Charlotte, Schuss Patrick, Güresir Erdem, Vatter Hartmut, Borger Valeri
Department of Neurosurgery, University Hospital Bonn, 53127 Bonn, Germany.
Department of Epileptology, University Hospital Bonn, 53127 Bonn, Germany.
Brain Sci. 2022 Jul 26;12(8):981. doi: 10.3390/brainsci12080981.
The aim of this study was the verification of the Subdural Hematoma in the Elderly (SHE) score proposed by Alford et al. as a mortality predictor in patients older than 65 years with nontraumatic/minor trauma acute subdural hematoma (aSDH). Additionally, we evaluated further predictors associated with poor outcome.
Patients were scored according to age (1 point is given if patients were older than 80 years), GCS by admission (1 point for GCS 5-12, 2 points for GCS 3-4), and SDH volume (1 point for volume 50 mL). The sum of points determines the SHE score. Multivariate logistic regression analysis was performed to identify additional independent risk factors associated with 30-day mortality.
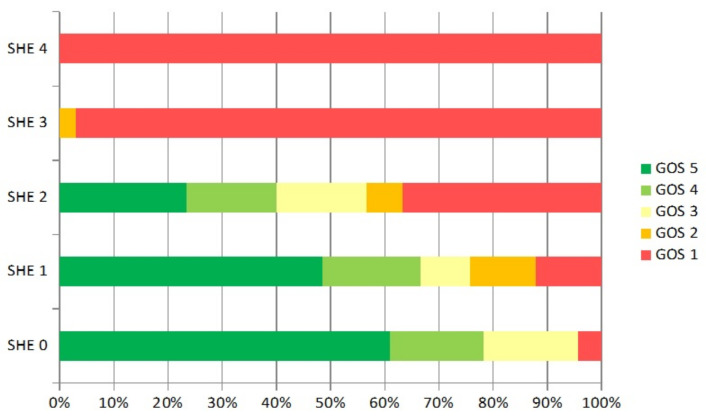
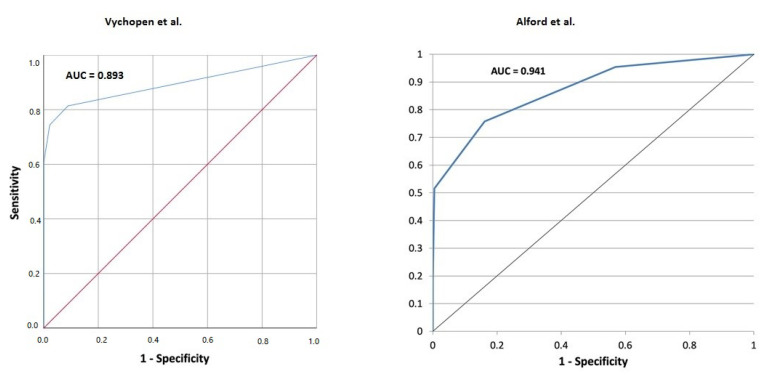
We evaluated 131 patients with aSDH who were treated at our institution between 2008 and 2020. We observed the same 30-day mortality rates published by Alford et al.: SHE 0: 4.3% vs. 3.2%, = 1.0; SHE 1: 12.2% vs. 13.1%, = 1.0; SHE 2: 36.6% vs. 32.7%, = 0.8; SHE 3: 97.1% vs. 95.7%, = 1.0 and SHE 4: 100% vs. 100%, = 1.0. Additionally, 18 patients who developed status epilepticus (SE) had a mortality of 100 percent regardless of the SHE score. The distribution of SE among the groups was: 1 for SHE 1, 6 for SHE 2, 9 for SHE 3, and 2 for SHE 4. The logistic regression showed the surgical evacuation to be the only significant risk factor for developing the seizure. All patients who developed SE underwent surgery ( = 0.0065). Furthermore, SHE 3 and 4 showed no difference regarding the outcome between surgical and conservative treatment.
SHE score is a reliable mortality predictor for minor trauma acute subdural hematoma in elderly patients. In addition, we identified status epilepticus as a strong life-expectancy-limiting factor in patients undergoing surgical evacuation.
本研究旨在验证阿尔福德等人提出的老年硬膜下血肿(SHE)评分,作为65岁以上非创伤性/轻度创伤急性硬膜下血肿(aSDH)患者的死亡率预测指标。此外,我们还评估了与不良预后相关的其他预测因素。
根据年龄(80岁以上患者得1分)、入院时的格拉斯哥昏迷量表(GCS)(GCS 5 - 12得1分,GCS 3 - 4得2分)和硬膜下血肿体积(体积≥50 mL得1分)对患者进行评分。分数总和决定SHE评分。进行多因素逻辑回归分析,以确定与30天死亡率相关的其他独立危险因素。
我们评估了2008年至2020年在我院接受治疗的131例aSDH患者。我们观察到与阿尔福德等人公布的30天死亡率相同:SHE 0:4.3%对3.2%,P = 1.0;SHE 1:12.2%对13.1%,P = 1.0;SHE 2:36.6%对32.7%,P = 0.8;SHE 3:97.1%对95.7%,P = 1.0;SHE 4:100%对100%,P = 1.0。此外,18例发生癫痫持续状态(SE)的患者,无论SHE评分如何,死亡率均为100%。SE在各分组中的分布情况为:SHE 1组1例,SHE 2组6例,SHE 3组9例,SHE 4组2例。逻辑回归显示手术清除是发生癫痫的唯一显著危险因素。所有发生SE的患者均接受了手术(P = 0.0065)。此外,SHE 3和SHE 4在手术治疗和保守治疗的预后方面无差异。
SHE评分是老年患者轻度创伤急性硬膜下血肿可靠的死亡率预测指标。此外,我们确定癫痫持续状态是接受手术清除的患者预期寿命的一个重要限制因素。