Marenghi Cristina, Qiu Zhuyu, Helleman Jozien, Nieboer Daan, Rubio-Briones Josè, Carroll Peter R, Lee Lui Shiong, Valdagni Riccardo, Boutros Paul C, Nicolai Nicola
Prostate Cancer Program, Fondazione IRCCS Istituto Nazionale dei Tumori, 20133 Milan, Italy.
Department of Human Genetics, University of California Los Angeles, Los Angeles, CA 90095, USA.
Cancers (Basel). 2022 Jul 22;14(15):3558. doi: 10.3390/cancers14153558.
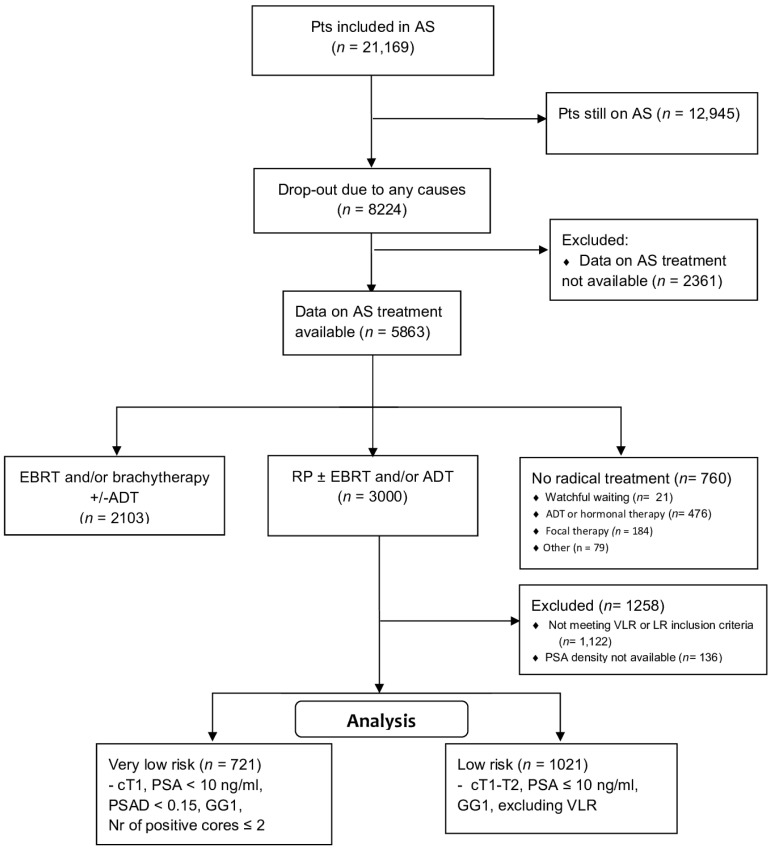
Background: Little is known about the consequences of delaying radical prostatectomy (RP) after Active Surveillance (AS) according to stringent or wider entry criteria. We investigated the association between inclusion criteria and rates, and timing of adverse pathological findings (APFs) among patients in GAP3 cohorts. Methods: APFs (GG ≥ 3, pT ≥ 3, pN > 0 and positive surgical margins [R1]) were accounted for in very low-risk (VLR: grade group [GG] 1, cT1, positive cores < 3, PSA < 10 ng/mL, PSA density [PSAD] < 0.15 ng/mL/cm3) and low-risk (LR: GG1, cT1-2, PSA ≤ 10 ng/mL) patients undergoing subsequent RP. The Kaplan−Meier method and log−rank test analyzed APF-free survival. Stratified mixed effects models analyzed association. Results: Out of 21,169 patients on AS, 1742 (VLR: 721; LR: 1021) underwent delayed RP. Most (60.8%) did not have APFs. APFs occurred more frequently (44.6% vs. 31.7%; OR 1.54, p < 0.001) and earlier (median time: 40.3 vs. 62.6 months; p < 0.001) in LR patients, and consisted of pT ≥ 3 (OR 1.47, p = 0.013) or R1 (OR 1.80, p < 0.001), but not of GG ≥ 3 or node involvement. Age (OR 1.05, p < 0.001), PSAD (OR 23.21, p = 0.003), and number of positive cores (OR 1.16, p = 0.004) were independently associated with APFs. Conclusions: AS stands as a safe option for low-risk patients, and most do not have APFs at surgery. Wider entry criteria are associated with pT3 and R1. The prognostic implications remain uncertain.
对于根据严格或更宽松的纳入标准在主动监测(AS)后延迟进行根治性前列腺切除术(RP)的后果知之甚少。我们调查了GAP3队列中患者的纳入标准与不良病理结果(APF)的发生率及时间之间的关联。方法:在接受后续RP的极低风险(VLR:分级组[GG]1,cT1,阳性核心<3,PSA<10 ng/mL,PSA密度[PSAD]<0.15 ng/mL/cm³)和低风险(LR:GG1,cT1 - 2,PSA≤10 ng/mL)患者中,对APF(GG≥3,pT≥3,pN>0和手术切缘阳性[R1])进行统计。采用Kaplan - Meier方法和对数秩检验分析无APF生存期。分层混合效应模型分析关联。结果:在21169例接受AS的患者中,1742例(VLR:721例;LR:1021例)接受了延迟RP。大多数(60.8%)没有APF。LR患者中APF出现得更频繁(44.6%对31.7%;OR 1.54,p<0.001)且更早(中位时间:40.3对62.6个月;p<0.001),并且包括pT≥3(OR 1.47,p = 0.013)或R1(OR 1.80,p<0.001),但不包括GG≥3或淋巴结受累。年龄(OR 1.05,p<0.001)、PSAD(OR 23.21,p = 0.003)和阳性核心数量(OR 1.16,p = 0.004)与APF独立相关。结论:AS对低风险患者是一种安全的选择,并且大多数患者在手术时没有APF。更宽松的纳入标准与pT3和R1相关。其预后意义仍不确定。