Department of Internal Medicine I.
Cirrhose Centrum Mainz (CCM), University Medical Center of the Johannes Gutenberg-University Mainz, Mainz.
Eur J Gastroenterol Hepatol. 2022 Oct 1;34(10):1053-1059. doi: 10.1097/MEG.0000000000002418. Epub 2022 Jul 21.
The liver is of critical importance for the homeostasis of metabolic and immunomodulatory properties as well as the storage of vitamins, especially vitamin A. In this prospective analysis, the incidence of serological vitamin A deficiency and the association with disease severity as well as clinical complications in patients with liver cirrhosis were investigated.
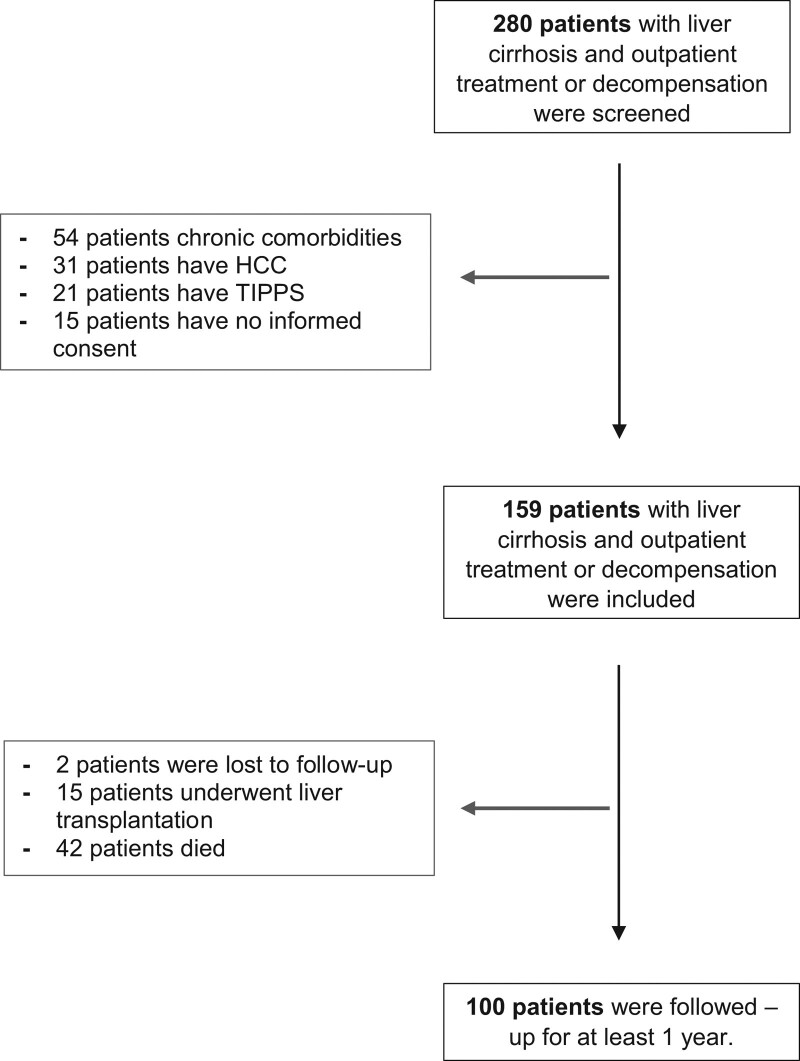
From May 2017 to May 2018, 159 patients with primarily alcohol-associated and non-alcoholic steatohepatitis (NASH)-associated preexisting liver cirrhosis were prospectively enrolled and vitamin A status was collected. Clinical complications and infections were followed and recorded over a period of 1-year follow-up. Selected findings were validated in an independent cohort of 44 patients.
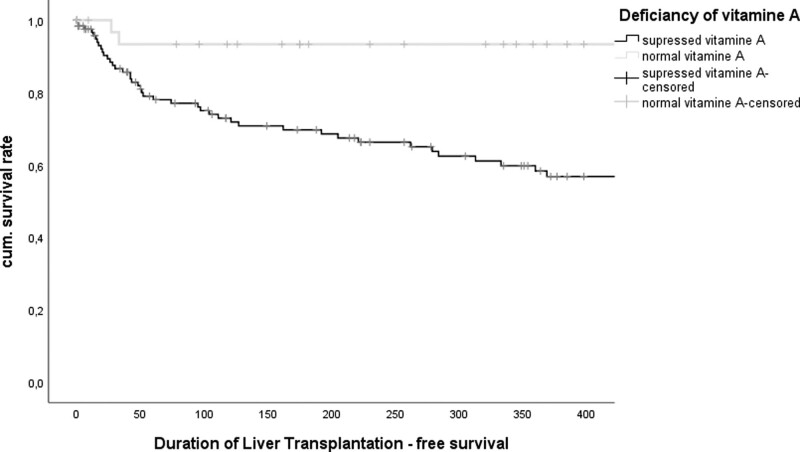
At study inclusion, 77% of patients showed decreased serological vitamin A. Suppressed vitamin A was more common in alcoholic (52 vs. 8%) and NASH-associated liver cirrhosis (16 vs. 9%) than in viral-associated liver cirrhosis. MELD score as well as Child-Pugh score were significantly associated with suppressed vitamin A ( P < 0.001). The association between the degree of vitamin A suppression and liver function was confirmed in univariate and multivariate regression analysis. After 1 year of follow-up, 57 patients died and 21 patients received a liver transplant. In addition, low vitamin A levels were more commonly observed in patients with severe ascites ( P = 0.001), hepatic encephalopathy ( P = 0.002) and hepatorenal syndromes ( P = 0.008). In addition, patients with reduced vitamin A showed an increased incidence of infections ( P = 0.02), especially respiratory infections ( P = 0.04).
Suppressed serological Vitamin A is common in patients with liver cirrhosis and is associated with liver function. Clinical complications and infections are more frequent in patients with liver cirrhosis and vitamin A suppression.
肝脏对于维持代谢和免疫调节特性以及储存维生素(尤其是维生素 A)至关重要。在这项前瞻性分析中,我们研究了肝硬化患者血清维生素 A 缺乏的发生率及其与疾病严重程度和临床并发症的关系。
从 2017 年 5 月至 2018 年 5 月,前瞻性地纳入了 159 例主要由酒精引起的和非酒精性脂肪性肝炎(NASH)引起的、先前存在的肝硬化患者,并收集了维生素 A 状况。对 1 年随访期间的临床并发症和感染进行随访和记录。在一个由 44 例患者组成的独立队列中验证了选定的发现。
在研究纳入时,77%的患者表现出血清维生素 A 降低。酒精性(52%比 8%)和 NASH 相关肝硬化(16%比 9%)比病毒性肝硬化更常见抑制性维生素 A。MELD 评分和 Child-Pugh 评分与抑制性维生素 A 显著相关(P<0.001)。在单变量和多变量回归分析中,维生素 A 抑制程度与肝功能之间的关系得到了证实。在 1 年的随访后,57 例患者死亡,21 例患者接受了肝移植。此外,在严重腹水(P=0.001)、肝性脑病(P=0.002)和肝肾综合征(P=0.008)患者中更常观察到低维生素 A 水平。此外,维生素 A 降低的患者感染发生率增加(P=0.02),特别是呼吸道感染(P=0.04)。
血清维生素 A 抑制在肝硬化患者中很常见,与肝功能有关。肝硬化和维生素 A 抑制患者的临床并发症和感染更为常见。