Center for Clinical Research, Vasteras, Faculty of Medicine, Uppsala University, Uppsala, Sweden.
Center for Clinical Research, Vasteras, Faculty of Medicine, Uppsala University, Uppsala, Sweden
BMJ Open. 2022 Jul 27;12(7):e057562. doi: 10.1136/bmjopen-2021-057562.
To assess the impact of total cholesterol (TC) and low-density lipoprotein cholesterol (LDL-C) on long-term all-cause mortality (ACM) in patients with acute myocardial infarction (AMI) and controls.
Matched case-control study with 8-year follow-up.
Vastmanland County Hospital, Vasteras, Sweden.
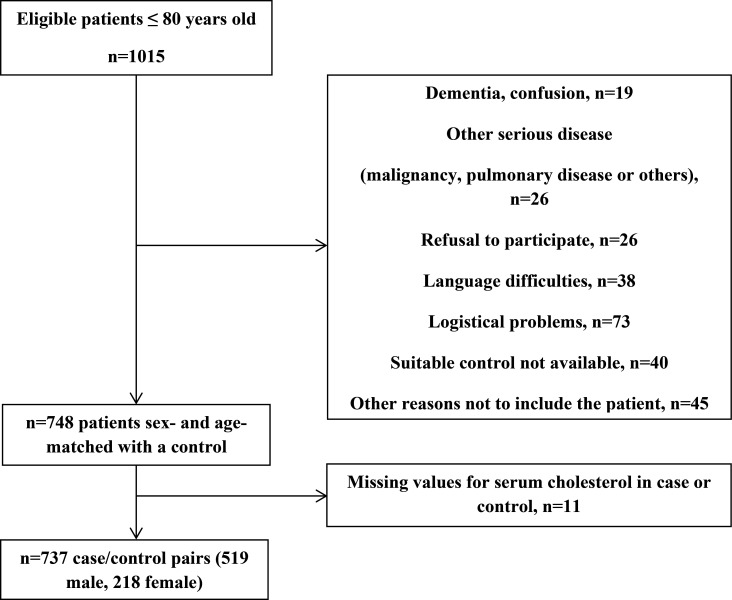
Consecutive patients with AMI admitted to the coronary care unit from March 2005 to May 2010 and age-matched and sex-matched controls from the general population.
ACM.
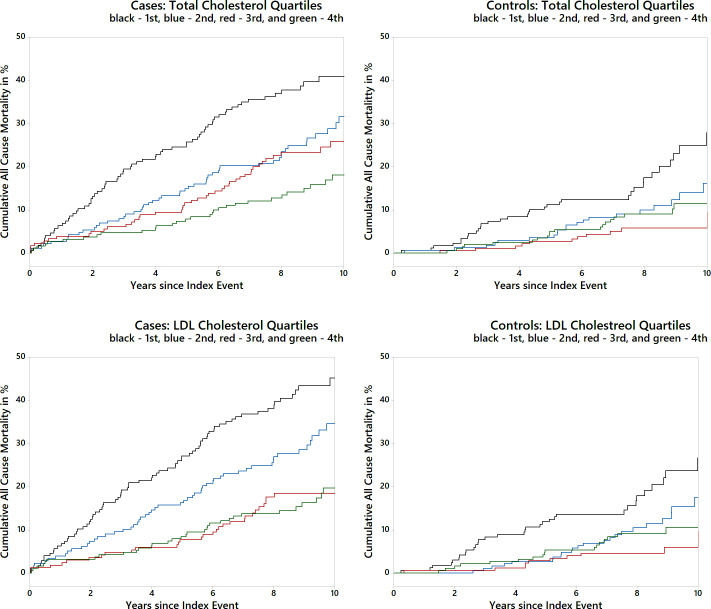
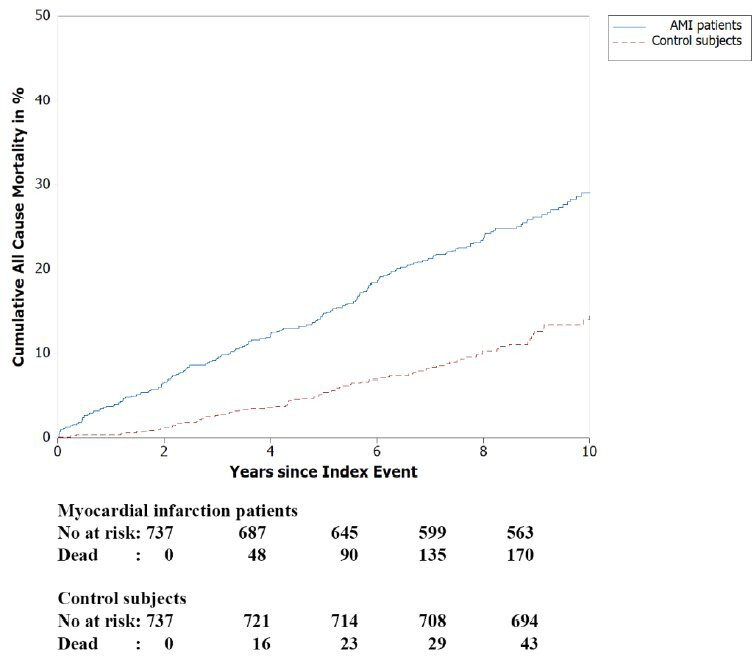
Person-year at risk among patients with AMI and controls was 11 667 (cases: 5780 and controls: 5887). During follow-up, 199 patients and 84 controls died, implying 3.4 deaths among patients and 1.4 among controls per 100 person-years at risk. Unadjusted Cox analyses showed significantly increasing mortality by decreasing TC and LDL-C levels in both patients (HR=0.70, 95% CI 0.62 to 0.79, p<0.001, and HR=0.64, 95% CI 0.56 to 0.74, p<0.001) and controls (HR=0.73, 95% CI 0.60 to 0.89, p=0.002, and HR=0.74, 95% CI 0.59 to 0.93, p=0.010). After adjusting for clinical variables, the results for the patients remained significant. Cox analyses of the relations between mortality and TC and LDL-C below and above their respective medians revealed the following pattern.
below medians were TC and LDL-C levels significantly inversely related to mortality; above medians there were no relations with mortality.
below medians were TC and LDL-C levels significantly inversely related to mortality; above medians were LDL-C levels significantly positively related to mortality. Mean LDL-C level in patients with blood sampled >12 hours after symptom onset was 0.41 mmol/L lower than that in patients with blood sampled ≤12 hours (p=0.030). This LDL-C decrease was reasonably caused by ongoing AMI and reflects the difference in LDL-C levels between patients and controls.
In patients with AMI, lower TC and LDL-C levels independently predict higher ACM. In their controls, LDL-C levels above the median independently predict higher ACM. This study adds to the body of evidence supporting the existence of a cholesterol paradox.
评估总胆固醇(TC)和低密度脂蛋白胆固醇(LDL-C)对急性心肌梗死(AMI)患者和对照者的长期全因死亡率(ACM)的影响。
具有 8 年随访的配对病例对照研究。
瑞典韦斯特罗斯县医院。
2005 年 3 月至 2010 年 5 月连续收治的 AMI 患者,以及来自普通人群的年龄和性别匹配的对照者。
ACM。
AMI 患者和对照者的风险人年为 11667 人年(病例组:5780 人年,对照组:5887 人年)。在随访期间,199 例患者和 84 例对照者死亡,意味着每 100 人年风险中有 3.4 例患者和 1.4 例对照者死亡。未校正的 Cox 分析显示,在患者(HR=0.70,95%CI 0.62 至 0.79,p<0.001 和 HR=0.64,95%CI 0.56 至 0.74,p<0.001)和对照者(HR=0.73,95%CI 0.60 至 0.89,p=0.002 和 HR=0.74,95%CI 0.59 至 0.93,p=0.010)中,TC 和 LDL-C 水平降低与死亡率呈显著正相关。在调整临床变量后,患者的结果仍有统计学意义。对死亡率与 TC 和 LDL-C 低于和高于各自中位数之间的关系进行 Cox 分析,结果显示如下。
TC 和 LDL-C 水平低于中位数与死亡率呈显著负相关;高于中位数时,与死亡率无相关性。
TC 和 LDL-C 水平低于中位数与死亡率呈显著负相关;高于中位数时,LDL-C 水平与死亡率呈显著正相关。发病后 12 小时以上采血的患者的平均 LDL-C 水平比发病后 12 小时内采血的患者低 0.41mmol/L(p=0.030)。这种 LDL-C 降低可能是由正在进行的 AMI 引起的,反映了患者和对照者之间 LDL-C 水平的差异。
在 AMI 患者中,TC 和 LDL-C 水平降低独立预测 ACM 较高。在其对照者中,LDL-C 水平高于中位数独立预测 ACM 较高。这项研究增加了支持胆固醇悖论存在的证据。