Nakajima Yuki, Nemoto Daiki, Nemoto Tetsutaro, Takahata Yosuke, Aizawa Masato, Utano Kenichi, Isohata Noriyuki, Endo Shungo, Lefor Alan Kawarai, Togashi Kazutomo
Department of Coloproctology, Aizu Medical Center Fukushima Medical University Fukushima Japan.
Department of Surgery Jichi Medical University Tochigi Japan.
DEN Open. 2022 Jun 16;3(1):e136. doi: 10.1002/deo2.136. eCollection 2023 Apr.
Endoscopic submucosal dissection (ESD) of colorectal lesions was invented in Japan, but postoperative management including hospital stay has not been reconsidered due to the Japanese insurance system. To explore appropriate postoperative management after colorectal ESD, we reviewed short-term outcomes after ESD in non-selected consecutive patients.
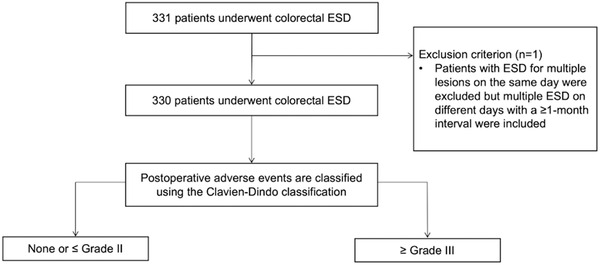
Patients who underwent colorectal ESD from April 2013 to September 2020 in one institution were reviewed. The primary outcome measure was the occurrence of adverse events stratified by the Clavien-Dindo classification with five grades. A logistic regression model with the Firth procedure was applied to investigate predictors of severe (grade III or greater) adverse events.
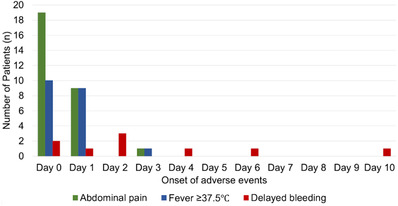
A total of 330 patients (female 40%, male 60%; median 72 years; IQR 65-80 years) with colorectal lesions (median 30 mm, IQR 23-40 mm; colon 77%, rectum 23%; serrated lesion 4%, adenoma 47%, mucosal cancer 30%, invasive cancer 18%) was evaluated. The en bloc resection rate was 97%. The median dissection time was 58 min (IQR: 38-86). Intraprocedural perforation occurred in 3%, all successfully treated by endoscopic clipping. No delayed perforations occurred. Postprocedural bleeding occurred in 3% on days 1-10 (median day 2); all were controlled endoscopically. Severe adverse events included only delayed bleeding. In analyzing severe adverse events in a multivariate logistic regression model with the Firth procedure, antithrombotic agent use ( = 0.016) and rectal lesions ( = 0.0010) were both significant predictors.
No serious adverse events occurred in this series. Four days of hospitalization may be too long for the majority of patients after ESD.
大肠病变的内镜黏膜下剥离术(ESD)是在日本发明的,但由于日本的保险制度,包括住院时间在内的术后管理尚未重新审视。为了探索大肠ESD术后的适当管理,我们回顾了非选择性连续患者ESD后的短期结果。
回顾了2013年4月至2020年9月在一家机构接受大肠ESD的患者。主要结局指标是根据Clavien-Dindo分类分为五个等级的不良事件的发生情况。应用带有Firth程序的逻辑回归模型来研究严重(III级或更高)不良事件的预测因素。
共评估了330例大肠病变患者(女性40%,男性60%;中位年龄72岁;四分位间距65 - 80岁)(中位病变大小30mm,四分位间距23 - 40mm;结肠77%,直肠23%;锯齿状病变4%,腺瘤47%,黏膜癌30%,浸润癌18%)。整块切除率为97%。中位剥离时间为58分钟(四分位间距:38 - 86)。术中穿孔发生率为3%,均通过内镜夹闭成功治疗。无延迟穿孔发生。术后1 - 10天(中位第2天)出血发生率为3%;均通过内镜控制。严重不良事件仅包括延迟出血。在使用Firth程序的多变量逻辑回归模型分析严重不良事件时,抗血栓药物使用(P = 0.016)和直肠病变(P = 0.0010)均为显著预测因素。
本系列中未发生严重不良事件。对于大多数ESD术后患者,四天的住院时间可能过长。