Takagi Tadataka, Kinoshita Shoichi, Kawaguchi Chihiro, Kojima Kuniyuki, Ueno Hirotsugu, Nishimura Naoki, Shimozato Naotaka, Shirai Yasuyo, Noguchi Ryuichi, Ohyama Takao
Department of Surgery Heisei Memorial Hospital Nara Japan.
Gut and Liver Center Heisei Memorial Hospital Nara Japan.
DEN Open. 2022 Jul 8;3(1):e145. doi: 10.1002/deo2.145. eCollection 2023 Apr.
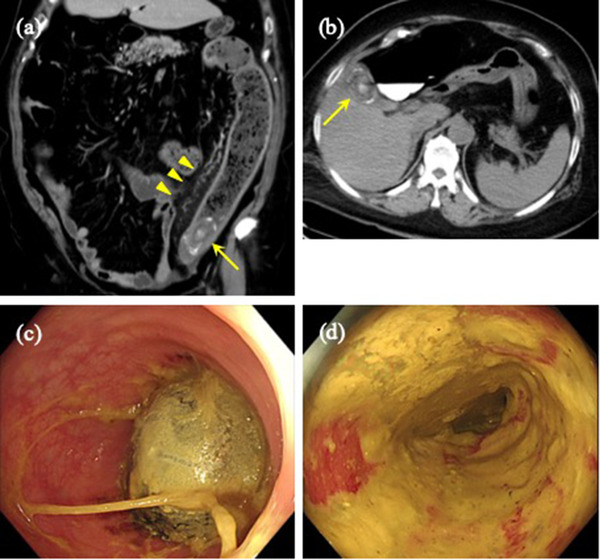
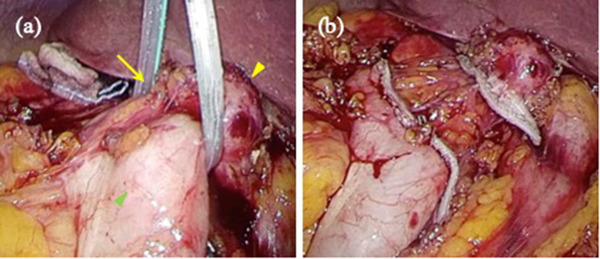
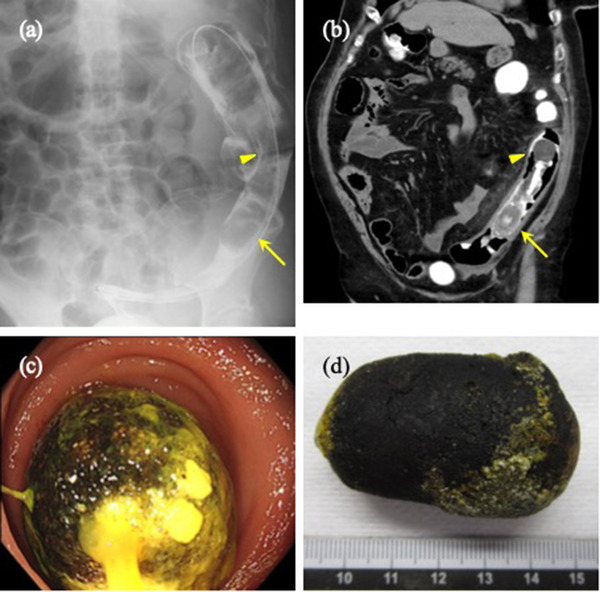
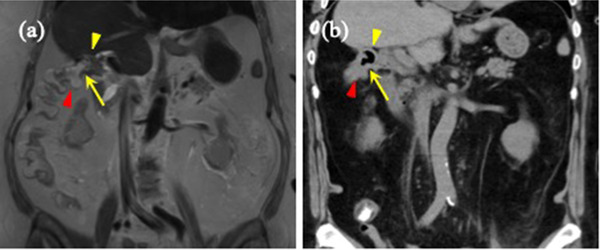
A 71-year-old obese woman was referred to our hospital with lower left abdominal pain. Computed tomography showed a 46 mm elliptic calcification lodged in the sigmoid-descending colon junction (SDJ), which had been detected 5 years prior but was not within the gall bladder at presentation. Therefore, we diagnosed colonic gallstone ileus with obstructive colitis caused by a gallstone. Colonoscopy revealed a smooth gallstone impacted at the sigmoid-descending colon junction, which was not fixed and could be pushed proximally with the endoscope. Dislodgement of the stone was unsuccessful with both a large polypectomy snare and a retrieval basket. Considering the high risk of surgery, we chose a non-surgical treatment strategy for obstructive colitis. Accordingly, a transanal ileus tube was placed to drain the proximal portion of the gallstone. The drainage of the colon by the ileus tube was satisfactory; the proximal colon was decompressed, ameliorating the obstructive colitis. Five days after tube placement, a colonoscopy revealed spontaneous passage of the gallstone into the rectum where it was finally removed. Cholecystocolonic fistula formation was confirmed by magnetic resonance imaging. We decided to surgically close the cholecystocolonic fistula to prevent future retrograde biliary infections. The surgery used a surgical stapler and was successful, with an uneventful postoperative course. Since radical surgical treatment of colonic gallstones and cholecystoenteric fistulas has a risk of postoperative morbidity and mortality, this case illustrates the importance of thoroughly considering nonsurgical interventions and surgeries for the safe treatment of colonic gallstone ileus.
一名71岁的肥胖女性因左下腹痛被转诊至我院。计算机断层扫描显示,在乙状结肠-降结肠交界处(SDJ)有一个46毫米的椭圆形钙化灶,该钙化灶在5年前就已被发现,但此次就诊时不在胆囊内。因此,我们诊断为结肠胆结石性肠梗阻伴胆结石引起的梗阻性结肠炎。结肠镜检查发现一枚光滑的胆结石嵌顿在乙状结肠-降结肠交界处,结石未固定,可在内镜下向近端推移。使用大型息肉切除圈套器和取石篮均未能成功取出结石。考虑到手术风险高,我们选择了针对梗阻性结肠炎的非手术治疗策略。因此,经肛门放置了一根肠梗阻导管以引流胆结石近端部分。肠梗阻导管对结肠的引流效果良好;近端结肠得以减压,梗阻性结肠炎有所改善。放置导管5天后,结肠镜检查显示胆结石自行排入直肠并最终取出。磁共振成像证实了胆囊结肠瘘的形成。我们决定通过手术封闭胆囊结肠瘘以防止未来发生逆行性胆道感染。手术使用了外科吻合器,手术成功,术后恢复顺利。由于结肠胆结石和胆囊肠瘘的根治性手术治疗有术后发病和死亡的风险,该病例说明了在安全治疗结肠胆结石性肠梗阻时充分考虑非手术干预和手术的重要性。