Taghlabi Khaled, Carlson Brandon B, Bunch Joshua, Jackson R Sean, Winfield Robert, Burton Douglas C
Department of Surgery, University of Kansas Medical Center, Kansas City, United States.
Department of Orthopedic Surgery, University of Kansas Medical Center, Kansas City, United States.
N Am Spine Soc J. 2022 Jul 12;11:100141. doi: 10.1016/j.xnsj.2022.100141. eCollection 2022 Sep.
Prophylactic anticoagulation is commonly used following operative treatment of spinal fractures to prevent Venous Thromboembolism (VTE) but carries a risk of bleeding complications. The purpose of the study was to compare VTE and bleeding complications for MID (≤72h) versus LATE (>72h) chemoprophylaxis timing after spinal fracture operative intervention.
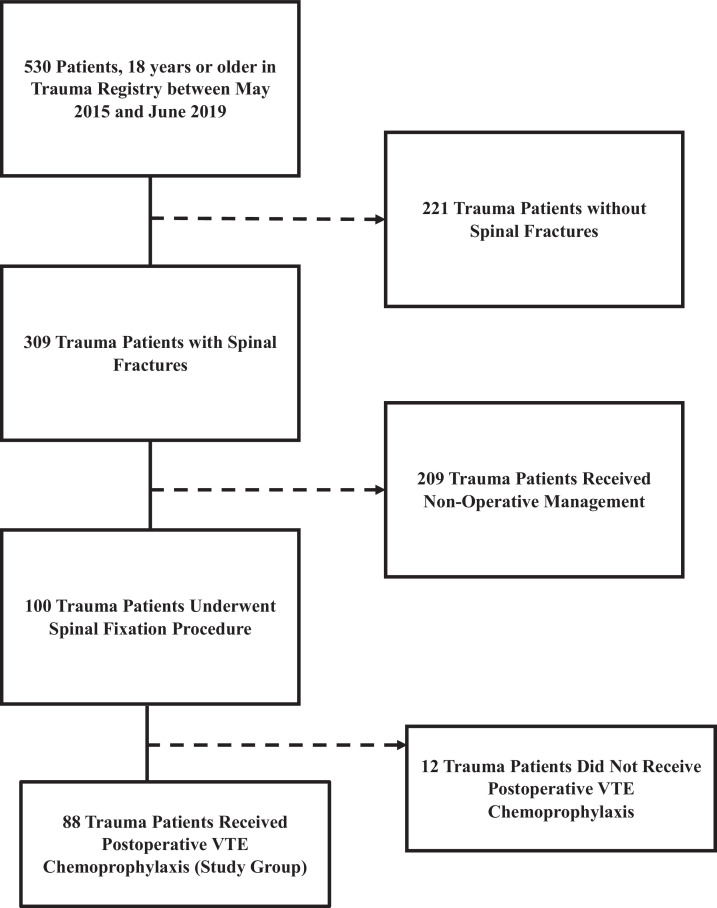
This is a retrospective review of patients treated for spinal fractures that received anticoagulation chemoprophylaxis between May 2015 and June 2019. Chemoprophylaxis initiation timing (MID vs. LATE) was the primary grouping variable. Patients with traumatic brain injury or evidence of intracranial or intraspinal bleed were excluded. Demographics, injury mechanisms, operative procedures, timing of administration of VTE prophylaxis, Injury Severity Score (ISS) and Spine Abbreviated Injury Scale (AIS), and complications including VTE and bleeding complications were collected. Predictors of VTE were identified using a binary logistic regression.
Eighty-eight patients (65M, 23F) met inclusion criteria. The median age was 55 years, and median Injury Severity Score (ISS) was 14. MID had 68 patients and LATE had 20. Nine patients developed VTE (6 LATE, 3 MID, 0.01. Three patients developed bleeding complications, and all occurred in the LATE group (0.01. ISS (<0.01) and GCS (<0.01) also correlated with an increased VTE rate.
Chemoprophylactic anticoagulation at 72 hours in surgically treated spinal fracture patients demonstrates a lower VTE rate without increasing complications. VTE prophylaxis can be initiated at 72 hours following spine fixation to decrease postinjury morbidity and mortality in this high-risk patient population.
脊柱骨折手术治疗后通常使用预防性抗凝治疗以预防静脉血栓栓塞症(VTE),但存在出血并发症风险。本研究旨在比较脊柱骨折手术干预后早期(≤72小时)与晚期(>72小时)化学预防时机的VTE和出血并发症情况。
这是一项对2015年5月至2019年6月期间接受抗凝化学预防治疗的脊柱骨折患者的回顾性研究。化学预防开始时机(早期与晚期)是主要分组变量。排除有创伤性脑损伤或颅内或脊柱内出血证据的患者。收集人口统计学、损伤机制、手术操作、VTE预防给药时机、损伤严重程度评分(ISS)和脊柱简明损伤量表(AIS)以及包括VTE和出血并发症在内的并发症。使用二元逻辑回归确定VTE的预测因素。
88例患者(65例男性,23例女性)符合纳入标准。中位年龄为55岁,中位损伤严重程度评分(ISS)为14分。早期组有68例患者,晚期组有20例。9例患者发生VTE(晚期组6例,早期组3例,P=0.01)。3例患者发生出血并发症,均发生在晚期组(P=0.01)。ISS(P<0.01)和格拉斯哥昏迷量表评分(GCS,P<0.01)也与VTE发生率增加相关。
手术治疗的脊柱骨折患者在72小时进行化学预防性抗凝显示VTE发生率较低且不增加并发症。脊柱固定术后72小时可开始VTE预防,以降低该高危患者群体的损伤后发病率和死亡率。