Department of Orthopaedics and Rehabilitation, Yale School of Medicine, New Haven, CT, United States of America.
Harvard Combined Orthopaedics Residency Program, Boston, MA, United States of America.
PLoS One. 2022 Jul 28;17(7):e0268215. doi: 10.1371/journal.pone.0268215. eCollection 2022.
Chondrosarcoma, although relatively uncommon, represents a significant percentage of primary osseous tumors. Nonetheless, there are few large-cohort, longitudinal studies of long-term survival and treatment outcomes of chondrosarcoma patients and none using the National Cancer Database (NCDB).
Chondrosarcoma patients were identified from the 2004-2015 NCDB datasets and divided on three primary tumor sites: appendicular, axial, and other. Demographic, treatment, and long-term survival data were determined for each group. Multivariate Cox analysis and Kaplan-Meier survival curves were generated to assess long-term survival over time for each.
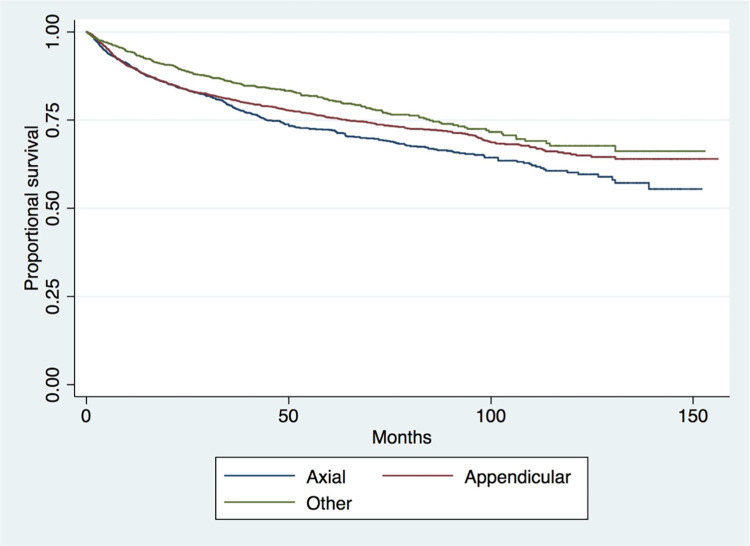
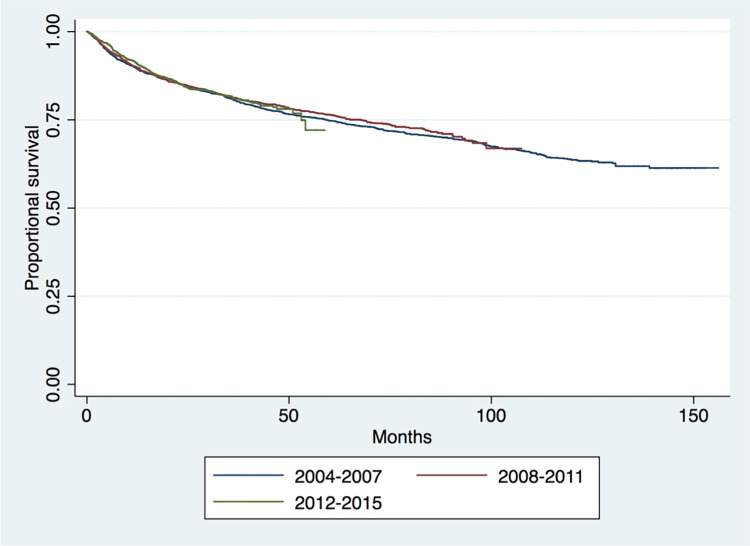
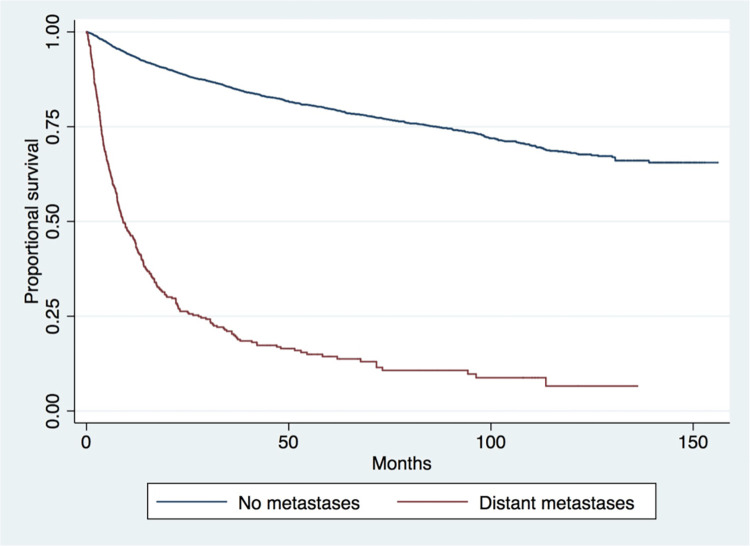
In total, 5,329 chondrosarcoma patients were identified, of which 2,686 were appendicular and 1,616 were axial. Survival was higher among the appendicular cohort than axial at 1-year, 5-year, and 10-year (89.52%, 75.76%, and 65.24%, respectively). Multivariate Cox analysis identified patients in the appendicular cohort to have significantly greater likelihood of death with increasing age category, distant metastases at presentation, and male sex (p<0.001 for each). Best outcomes for seen for those undergoing surgical treatment (p<0.001). Patients in the axial cohort were with increased likelihood of death with increasing age category and distant metastases (p<0.001), while surgical treatment with or without radiation were associated with a significant decrease (p<0.001). Kaplan-Meier survival analysis showed worst survival for the axial cohort (p<0.001) and patients with distant metastases at presentation (p<0.001). Survival was not significantly different between older (2004-2007) and more recent years (2012-2016) (p = 0.742).
For both appendicular and axial chondrosarcomas, surgical treatment remains the mainstay of treatment due to its continued superiority for the long-term survival of patients, although advancements in survival over the last decade have been insignificant. Presence of distant metastases and axial involvement are significant, poor prognostic factors perhaps because of difficulty in surgical excision or extent of disease.
尽管软骨肉瘤相对少见,但它是原发性骨肿瘤的重要组成部分。然而,目前很少有大型的、长期的、针对软骨肉瘤患者生存和治疗结果的队列研究,也没有使用国家癌症数据库(NCDB)的研究。
从 2004 年至 2015 年的 NCDB 数据集确定了软骨肉瘤患者,并根据三个主要肿瘤部位进行了分类:四肢、轴性和其他。确定了每个组的人口统计学、治疗和长期生存数据。使用多变量 Cox 分析和 Kaplan-Meier 生存曲线来评估每个部位的长期生存情况。
总共确定了 5329 例软骨肉瘤患者,其中 2686 例为四肢,1616 例为轴性。在 1 年、5 年和 10 年时,四肢部位的生存率高于轴性部位(分别为 89.52%、75.76%和 65.24%)。多变量 Cox 分析确定,随着年龄类别、就诊时远处转移和男性的增加,四肢部位的患者死亡的可能性显著增加(p<0.001)。手术治疗的患者预后最佳(p<0.001)。轴性部位的患者随着年龄类别和远处转移的增加,死亡的可能性增加(p<0.001),而手术治疗加或不加放疗与显著降低(p<0.001)相关。Kaplan-Meier 生存分析显示,轴性部位的生存最差(p<0.001),就诊时存在远处转移的患者生存最差(p<0.001)。与较老的年份(2004-2007 年)相比,较新的年份(2012-2016 年)的生存情况无显著差异(p = 0.742)。
对于四肢和轴性软骨肉瘤,手术治疗仍然是治疗的主要方法,因为它继续为患者的长期生存提供优势,尽管过去十年的生存进展微不足道。远处转移和轴性受累是显著的、预后不良的因素,这可能是由于手术切除的困难或疾病的严重程度。