Ruiz Department of Ophthalmology and Visual Science, McGovern Medical School, The University of Texas Health Science Center (UTHealth).
Robert Cizik Eye Clinic.
J Glaucoma. 2022 Sep 1;31(9):701-709. doi: 10.1097/IJG.0000000000002079. Epub 2022 Jul 21.
Short-term overall success rates were high with either SGDD or CPC. However, SGDD was associated with more clinic visits and an increased risk of additional glaucoma surgery. Both treatments were reasonable options for eyes with inadequately controlled IOP after a single GDD.
The purpose of this study is to compare the implantation of a second glaucoma drainage device (SGDD) and transscleral cyclophotocoagulation (CPC) in eyes with inadequately controlled intraocular pressure (IOP), despite the presence of a preexisting glaucoma drainage device.
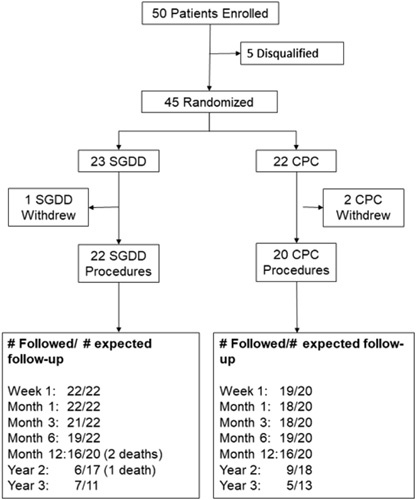
Patients with inadequately controlled IOP, despite the medical therapy and a preexisting glaucoma drainage device, were enrolled at 14 clinical centers and randomly assigned to treatment with a SGDD or CPC.
Surgical failure was defined as: (1) IOP ≤5 mm Hg or >18 mm Hg or <20% reduction below baseline on maximum tolerated topical ocular hypotensive therapy, (2) reoperation for glaucoma, or (3) loss of light perception. The primary outcome measure was overall success with or without adjunctive medical therapy.
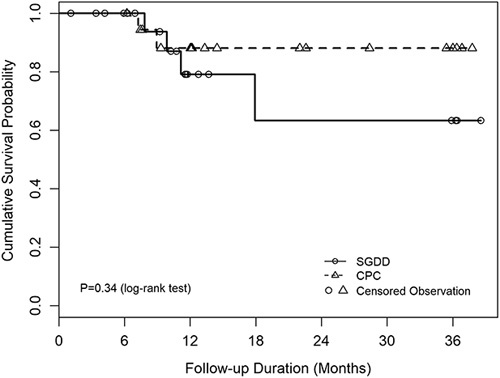
Forty-two eyes of 42 participants were randomized to SGDD (n=22) or CPC (n=20). Mean duration of follow-up was 18.6 (±12.1; range: 1.1-38.6) months. The cumulative success rate was 79% for SGDD and 88% for CPC at 1 year ( P =0.63). Although the study was underpowered, no significant differences in IOP, postoperative number of IOP-lowering medications, or adverse events were observed. The number of additional glaucoma surgeries ( P =0.003), office visits during the first 3 months ( P <0.001), and office visits per month after month 3 ( P <0.001) were greater in the SGDD group.
Short-term overall success rates were high with either SGDD or CPC. However, SGDD was associated with more clinic visits and an increased risk of additional glaucoma surgery.
尽管存在预先存在的青光眼引流装置,但短期总体成功率在 SGDD 或 CPC 中均较高。然而,SGDD 与更多的就诊次数和增加的额外青光眼手术风险相关。对于眼压控制不佳的单眼,这两种治疗方法都是合理的选择。
本研究旨在比较植入第二只青光眼引流装置(SGDD)和经巩膜睫状体光凝(CPC)在眼压(IOP)控制不佳的情况下,尽管存在预先存在的青光眼引流装置。
在 14 个临床中心招募了眼压控制不佳的患者,尽管进行了药物治疗和预先存在的青光眼引流装置,但他们被随机分配接受 SGDD 或 CPC 治疗。
手术失败定义为:(1)IOP≤5mmHg 或>18mmHg 或与基线相比最大耐受局部降眼压治疗降低<20%,(2)因青光眼再次手术,或(3)光感丧失。主要观察指标为不联合辅助药物治疗的总体成功率。
42 名参与者的 42 只眼被随机分配到 SGDD(n=22)或 CPC(n=20)。平均随访时间为 18.6(±12.1;范围:1.1-38.6)个月。SGDD 的 1 年累积成功率为 79%,CPC 为 88%(P=0.63)。尽管研究样本量不足,但观察到 IOP、术后降眼压药物数量或不良事件无显著差异。SGDD 组的额外青光眼手术数量(P=0.003)、前 3 个月的就诊次数(P<0.001)和第 3 个月后每月的就诊次数(P<0.001)更多。
短期总体成功率在 SGDD 或 CPC 中均较高。然而,SGDD 与更多的就诊次数和增加的额外青光眼手术风险相关。