Department of General Surgery, Beijing Chao-Yang Hospital, Capital Medical University, Beijing, China.
Department of Radiology, Beijing Chao-Yang Hospital, Capital Medical University, Beijing, China.
Cancer Med. 2023 Feb;12(3):2440-2452. doi: 10.1002/cam4.5076. Epub 2022 Jul 29.
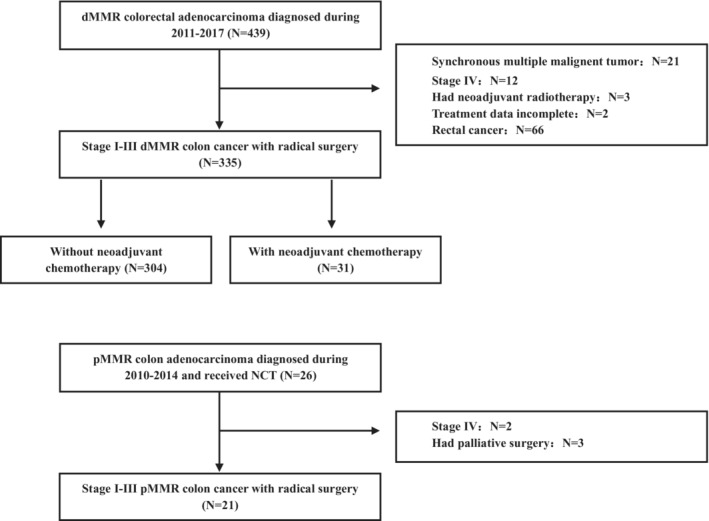
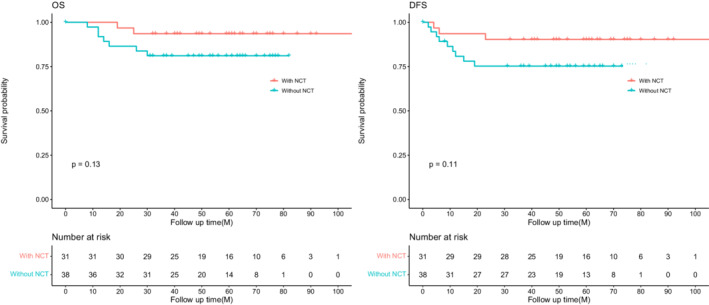
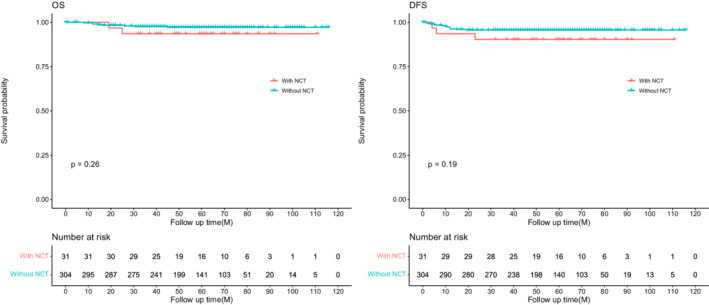
Colon cancers with mismatch repair deficiency (dMMR) have specific clinicopathologic characteristics compared with mismatch repair proficiency (pMMR); however, the effect of MMR status on the efficiency of neoadjuvant chemotherapy (NCT) remains unclear. In our study, 439 dMMR and 26 pMMR colon cancer patients with or without NCT from 2010 to 2017 were retrospectively collected. Clinicopathological features, treatment response, and survival were compared between different groups. In the dMMR group, patients with NCT were likely to have higher CEA (abnormal CEA: 51.6% vs. 17.4%, p < 0.001), more multiorgan resection (38.7% vs. 16.8%, p = 0.006), and larger postoperative tumor diameter (7.26 vs. 6.21, p = 0.033) than those without NCT, but nearly half of cT4b patients who had NCT (42.9%, 9/21) avoid multiorgan resection. pT4 stage (HR, 14.97; 95% CI, 1.88-118.92; p = 0.010), number of positive lymph nodes (HR, 1.17; 95% CI, 1.09-1.26; p < 0.001), and tumor deposit (HR, 6.73; 95% CI, 2.08-21.74; p = 0.001) were independent prognosis factors of disease-free survival (DFS). For the advanced tumor subset, there is no significant difference between patients with or without NCT for OS (p = 0.13) and DFS (p = 0.11), although the survival rate of NCT was higher than non-NCT patients. Moreover, tumor regression grade was similar between dMMR and pMMR patients who had NCT. This study showed that NCT was more likely to be employed in dMMR patients with advanced tumors and may reduce the rate of multiorgan resection for cT4b dMMR patients. More large-scaled researches are needed to further explore if MMR status could predict the efficacy of neoadjuvant chemotherapy in patients with colon cancer.
错配修复缺陷(dMMR)的结肠癌与错配修复功能正常(pMMR)的结肠癌相比具有特定的临床病理特征;然而,MMR 状态对新辅助化疗(NCT)效率的影响仍不清楚。在我们的研究中,回顾性收集了 2010 年至 2017 年期间有或没有 NCT 的 439 例 dMMR 和 26 例 pMMR 结肠癌患者。比较了不同组之间的临床病理特征、治疗反应和生存情况。在 dMMR 组中,接受 NCT 的患者更可能出现更高的 CEA(异常 CEA:51.6% vs. 17.4%,p<0.001)、更多的多器官切除(38.7% vs. 16.8%,p=0.006)和更大的术后肿瘤直径(7.26 vs. 6.21,p=0.033),但近一半的 cT4b 患者接受了 NCT(42.9%,9/21)避免了多器官切除。pT4 期(HR,14.97;95%CI,1.88-118.92;p=0.010)、阳性淋巴结数(HR,1.17;95%CI,1.09-1.26;p<0.001)和肿瘤沉积(HR,6.73;95%CI,2.08-21.74;p=0.001)是无病生存(DFS)的独立预后因素。对于晚期肿瘤亚组,接受或未接受 NCT 的患者的 OS(p=0.13)和 DFS(p=0.11)无显著差异,尽管 NCT 患者的生存率高于非 NCT 患者。此外,接受 NCT 的 dMMR 和 pMMR 患者的肿瘤消退分级相似。这项研究表明,NCT 更有可能用于晚期 dMMR 患者,并且可能降低 cT4b dMMR 患者的多器官切除率。需要更多的大规模研究来进一步探讨 MMR 状态是否可以预测结肠癌患者新辅助化疗的疗效。