Division of Cardiology, Department of Internal Medicine, Hanyang University College of Medicine, 222 Wangsimni-ro, Sungdong-gu, Seoul, 04763, Republic of Korea.
Department of Cardiology, Hanyang University Guri Hospital, Gyeong-Choon Street 153, Guri, Gyounggido, Republic of Korea.
Sci Rep. 2022 Jul 29;12(1):12996. doi: 10.1038/s41598-022-16631-3.
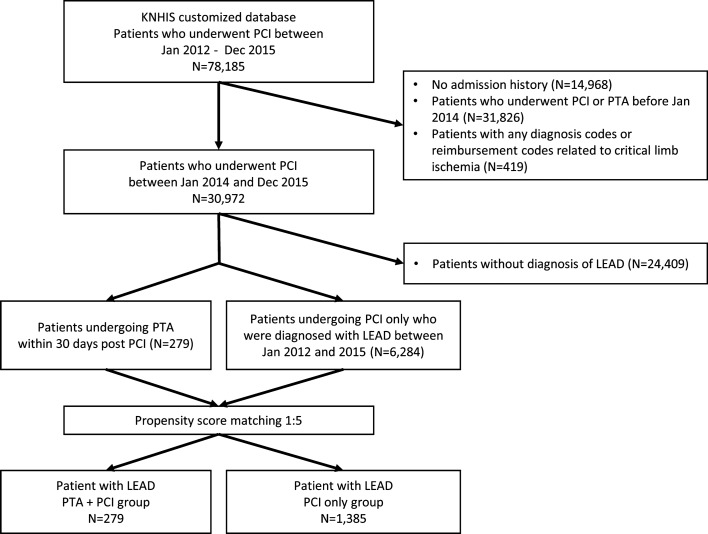
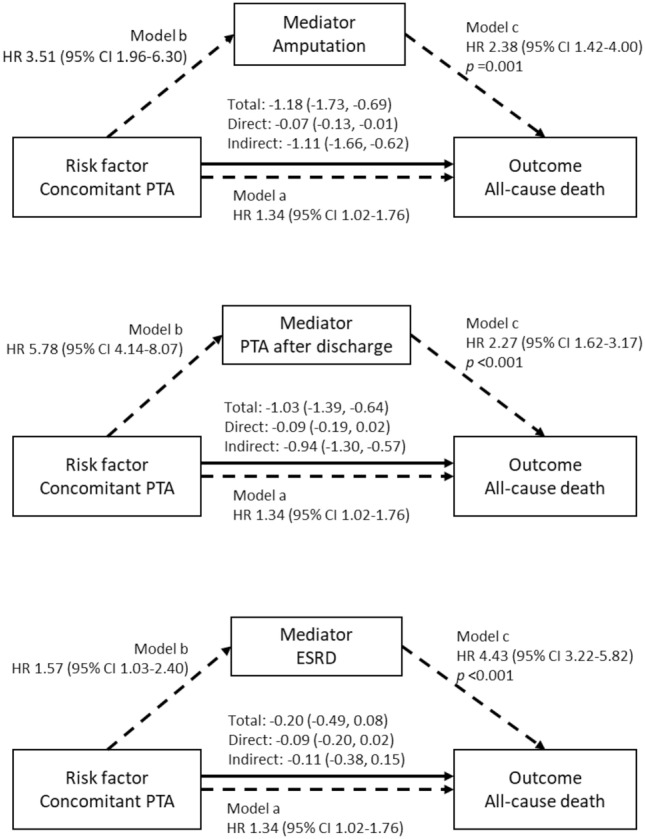
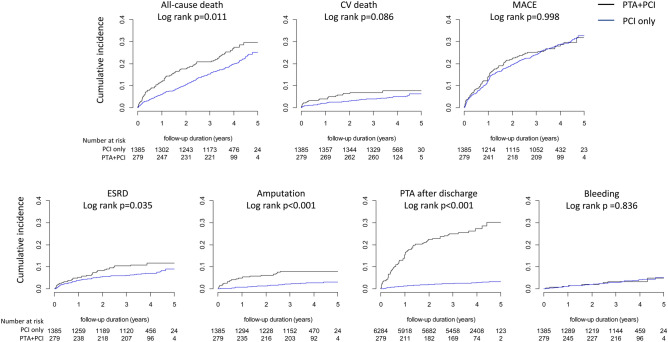
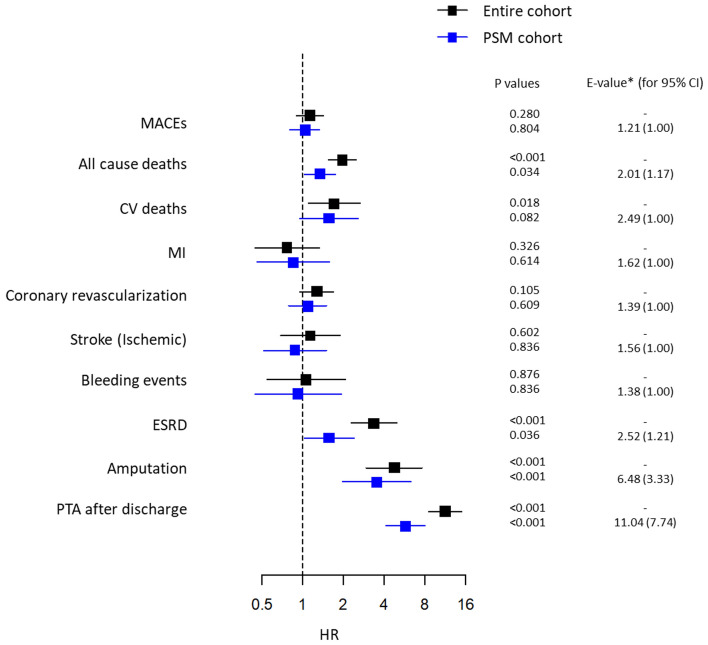
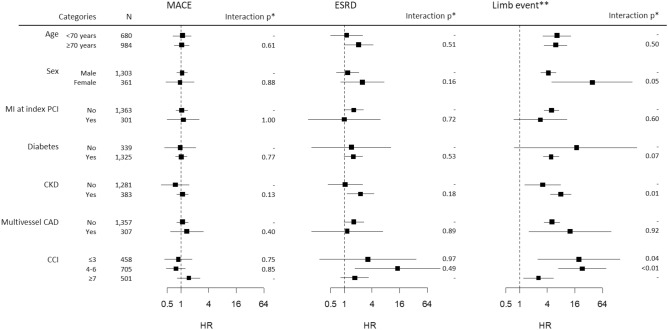
Concomitant percutaneous transluminal angioplasty (PTA) at the time of percutaneous coronary intervention (PCI) is often performed because lower extremity artery disease (LEAD) commonly coincides with coronary artery disease. We investigated the impact of concomitant PTA on both cardiovascular and limb outcomes in the Korean National Health Insurance Service registry. Among 78,185 patients undergoing PCI, 6563 patients with stable LEAD without limb ischemia were included. After 1:5 propensity score matching was conducted, 279 patients in the PTA + PCI group and 1385 patients in the PCI group were compared. Multivariate Cox proportional hazard models showed that the risk of all-cause death was higher in the PTA + PCI group than in the PCI group, whereas the risks of myocardial infarction, repeat revascularization, stroke, cardiovascular death and bleeding events were not different between the 2 groups. In contrast, the risks of end-stage renal disease and unfavorable limb outcomes were higher in the PTA + PCI group. Mediation analyses revealed that amputation and PTA after discharge significantly mediated the association between concomitant PTA and all-cause death. Concomitant PTA was not associated with an increased risk of cardiovascular events but may increase the risk of all-cause death mediated by unfavorable renal and limb outcomes in patients with stable LEAD.
同期经皮腔内血管成形术(PTA)在经皮冠状动脉介入治疗(PCI)时经常进行,因为下肢动脉疾病(LEAD)通常与冠状动脉疾病同时存在。我们在韩国国家健康保险服务登记处调查了同期 PTA 对心血管和肢体结局的影响。在接受 PCI 的 78185 名患者中,纳入了 6563 名无肢体缺血的稳定型 LEAD 患者。在进行了 1:5 的倾向评分匹配后,比较了 PTA+PCI 组的 279 名患者和 PCI 组的 1385 名患者。多变量 Cox 比例风险模型显示,PTA+PCI 组的全因死亡风险高于 PCI 组,而两组之间心肌梗死、再次血运重建、卒中和心血管死亡以及出血事件的风险无差异。相比之下,PTA+PCI 组的终末期肾病和不良肢体结局的风险更高。中介分析表明,截肢和出院后的 PTA 显著介导了同期 PTA 与全因死亡之间的关联。同期 PTA 与心血管事件的风险增加无关,但可能会增加稳定型 LEAD 患者不良肾脏和肢体结局介导的全因死亡风险。