Division of Nephrology, The Second Hospital of Jilin University, Changchun, China.
Division of Nephrology, The First Hospital of Jilin University-the Eastern Division, Changchun, China.
Front Endocrinol (Lausanne). 2022 Jul 14;13:936573. doi: 10.3389/fendo.2022.936573. eCollection 2022.
The optimal break-in period (BI) of urgent-start peritoneal dialysis (USPD) initiation for patients with end-stage renal disease (ESRD) and diabetes is unclear. We aimed to explore the safety and applicability of a BI ≤24 h in patients with ESRD and diabetes.
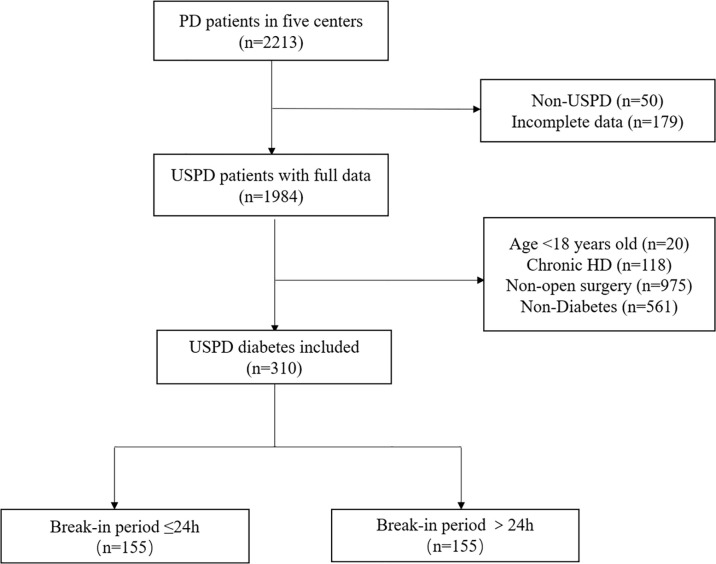
We used a retrospective cohort design wherein we recruited patients with ESRD and diabetes who underwent USPD at five institutions in China between January 2013 and August 2020. The enrolled patients were grouped according to BI. The primary outcomes were mechanical and infectious complication occurrences, whereas the secondary outcome was technique survival.
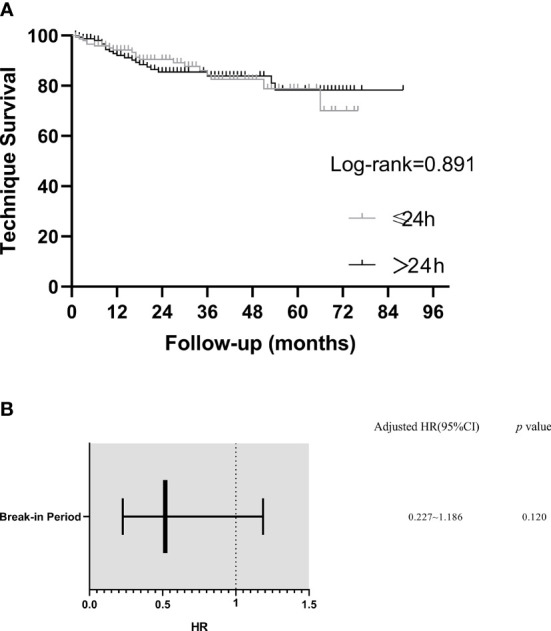
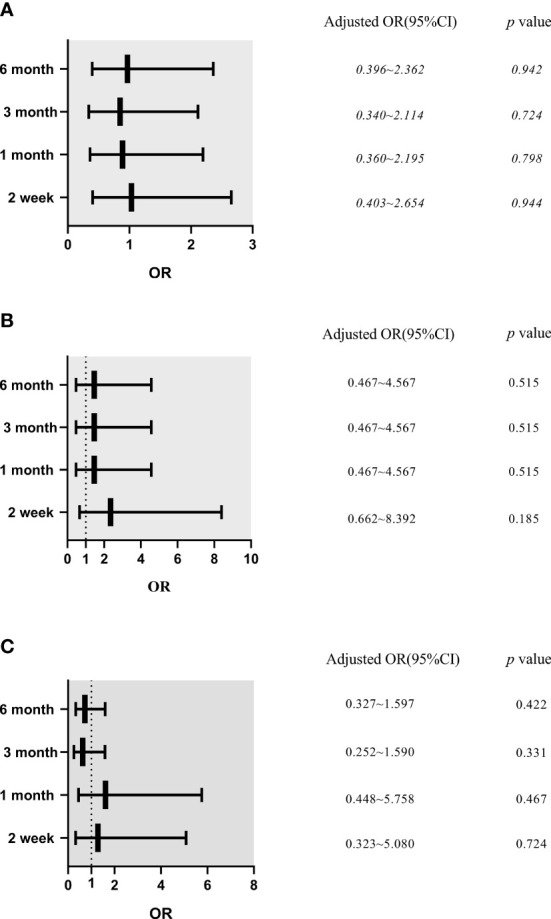
We enrolled 310 patients with diabetes, of whom 155 and 155 patients were in the BI ≤24 h and BI >24 h groups, respectively. The two groups showed a comparable incidence of infectious and mechanical complications within 6 months after catheter insertion (>0.05). Logistic regression analysis revealed that a BI ≤24 h was not an independent risk factor for mechanical or infectious complications. Kaplan-Meier estimates showed no statistically significant between-group differences in technique survival rates (>0.05). Cox multivariate regression analysis revealed that a BI ≤24 h was not an independent risk factor for technique failure.
USPD initiation with a BI ≤24 h may be safe and feasible for patients with ESRD and diabetes.
终末期肾病(ESRD)合并糖尿病患者行紧急起始持续性不卧床腹膜透析(USPD)的最佳起始过渡期(BI)尚不明确。本研究旨在探索 ESRD 合并糖尿病患者 BI≤24 小时的安全性和适用性。
本研究采用回顾性队列设计,纳入 2013 年 1 月至 2020 年 8 月期间在中国 5 家中心行 USPD 的 ESRD 合并糖尿病患者。根据 BI 将患者分为 BI≤24 小时组和 BI>24 小时组。主要结局为机械性和感染性并发症的发生情况,次要结局为技术生存率。
本研究共纳入 310 例糖尿病患者,其中 BI≤24 小时组和 BI>24 小时组各 155 例。两组患者在导管置入后 6 个月内的感染和机械性并发症发生率相近(>0.05)。Logistic 回归分析显示 BI≤24 小时不是机械性或感染性并发症的独立危险因素。Kaplan-Meier 估计显示两组患者的技术生存率无统计学差异(>0.05)。Cox 多因素回归分析显示 BI≤24 小时不是技术失败的独立危险因素。
对于 ESRD 合并糖尿病患者,起始 USPD 时 BI≤24 小时可能是安全且可行的。