Stäuble Céline K, Meier Rebecca, Lampert Markus L, Mikoteit Thorsten, Hatzinger Martin, Allemann Samuel S, Hersberger Kurt E, Meyer Zu Schwabedissen Henriette E
Biopharmacy, Department of Pharmaceutical Sciences, University of Basel, Basel, Switzerland.
Pharmaceutical Care, Department of Pharmaceutical Sciences, University of Basel, Basel, Switzerland.
Front Psychiatry. 2022 Jul 15;13:942268. doi: 10.3389/fpsyt.2022.942268. eCollection 2022.
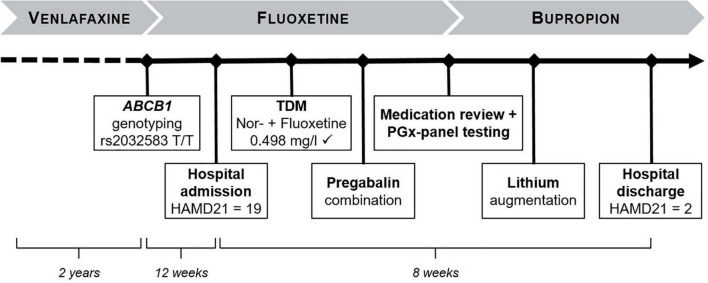
We report the case of a 50-year-old male with major depressive disorder (MDD) to illustrate the challenge of finding effective antidepressant pharmacotherapy and the role that the patient's genetic makeup may play. Recent treatment attempts before clinic admission included venlafaxine and fluoxetine. Venlafaxine was discontinued due to lack of response, and subsequently switched to fluoxetine based on pharmacogenotyping of the P-glycoprotein transporter (P-gp, encoded by ) by the outpatient psychiatrist. Despite steady state serum levels within the therapeutic range, the patient did not benefit from fluoxetine either, necessitating admission to our clinic. Here a clinical pharmacist-led medication review including additional pharmacogenetic (PGx) analysis resulted in the change of the antidepressant therapy to bupropion. Under the new regimen, established in the in-patient-setting, the patient remitted. However, based on the assessed pharmacokinetics-related gene variants, including s and , non-response to fluoxetine could not be conclusively explained. Therefore, we retrospectively selected the serotonin transporter (SERT1, encoded by ) for further genetic analysis of pharmacodynamic variability. The patient presented to be a homozygous carrier of the short allele variant in the 5-HTTLPR (S/S) located within the promoter region, which has been associated with a reduced expression of the SERT1. This case points out the potential relevance of panel PGx testing considering polymorphisms in genes of pharmacokinetic as well as pharmacodynamic relevance.
我们报告了一例50岁患有重度抑郁症(MDD)的男性病例,以说明寻找有效的抗抑郁药物治疗方法所面临的挑战以及患者基因构成可能发挥的作用。入院前最近的治疗尝试包括使用文拉法辛和氟西汀。由于没有反应,文拉法辛被停用,随后门诊精神科医生根据P-糖蛋白转运体(P-gp,由 编码)的药物基因分型将其换用氟西汀。尽管稳态血清水平在治疗范围内,但患者也未从氟西汀中获益,因此需要入住我们的诊所。在这里,由临床药剂师主导的药物审查包括额外的药物遗传学(PGx)分析,结果将抗抑郁治疗改为安非他酮。在住院期间确定的新治疗方案下,患者病情缓解。然而,基于评估的与药代动力学相关的基因变异,包括 s和 ,无法确凿解释对氟西汀无反应的原因。因此,我们回顾性地选择了血清素转运体(SERT1,由 编码)进行药效学变异性的进一步基因分析。该患者在位于 启动子区域的5-HTTLPR中呈现为短等位基因变体的纯合携带者(S/S),这与SERT1表达降低有关。该病例指出了考虑药代动力学和药效学相关基因多态性的综合PGx检测的潜在相关性。