Division Of Pediatric Surgery, Department Of Surgery, Faculty Of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand.
Pediatric Surgery Unit, Department of Surgery, Khon Kaen University, Khon Kaen, Thailand.
BMC Pediatr. 2022 Aug 3;22(1):467. doi: 10.1186/s12887-022-03524-7.
Findings from manometry studies and contrast imaging reveal functioning gastric physiology in newborns with duodenal atresia and stenosis. Stomach reservoir function should therefore be valuable in aiding the postoperative phase of gastric feeding. The aim of this study was therefore to compare the feasibility of initiating oral or large volume(s) gavage feeds vs small volume bolus feeds following operation for congenital duodenal anomalies.
Single-center electronic medical records of all babies with duodenal atresia and stenosis admitted to a university surgical center during January 1997-September 2021 were analyzed. A fast-fed group (FF) included newborns fed with oral or gavage feeds advanced at a rate of at least 2.5 ml/kg and then progressed more than once a day vs slow-fed group (SF) fed with gavage feeds at incremental rate less than 2.5 ml/kg/day for each time period of oral tolerance or by drip feeds. Total feed volume was limited to 120-150 ml/kg/day in the respective study cohort populations.
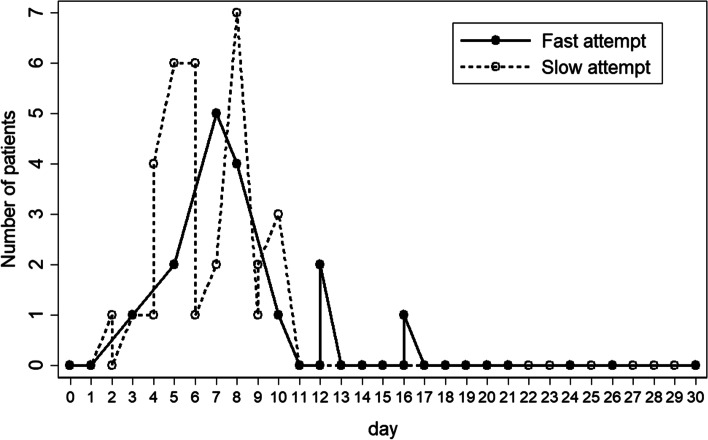
Fifty-one eligible patients were recruited in the study - twenty-six in FF group and twenty-five in SF group. Statistically significant differences were observed in the (i) date of first oral feeds (POD 7.7 ± 3.2 vs 16.1 ± 7.7: p < 0.001), and (ii) first full feeds (POD 12.5 ± 5.3 vs 18.8 ± 9.7: p < 0.01) in FF vs SF study groups.
Initial feeding schedules with oral or incremental gavage-fed rates of at least 2.5 ml/kg in stepwise increments and multi-steps per day is wholly feasible in the postoperative feeding regimens of neonates with congenital duodenal disorders. Significant health benefits are thus achievable in these infants allowing an earlier time to acquiring full enteral feeding and their hospital discharge.
测压研究和对比成像的结果揭示了先天性十二指肠闭锁和狭窄新生儿的胃功能正常。因此,胃储留功能对于辅助胃喂养的术后阶段应该是有价值的。本研究的目的是比较在先天性十二指肠畸形手术后,通过口服或大体积(s)胃管喂养与小体积推注喂养启动胃喂养的可行性。
分析了 1997 年 1 月至 2021 年 9 月期间在一家大学外科中心收治的所有患有先天性十二指肠闭锁和狭窄的婴儿的单中心电子病历。快速喂养组(FF)包括以至少 2.5ml/kg 的速度经口或胃管喂养,并每天至少增加一次喂养的新生儿,而缓慢喂养组(SF)则以每天递增的方式经胃管喂养,增量小于 2.5ml/kg/天,每次根据口服耐受或滴注喂养的情况而定。在各自的研究队列人群中,总喂养量限制在 120-150ml/kg/天。
本研究共纳入 51 例符合条件的患者,FF 组 26 例,SF 组 25 例。FF 组与 SF 组在(i)首次口服喂养时间(POD 7.7±3.2 与 16.1±7.7:p<0.001)和(ii)首次完全喂养时间(POD 12.5±5.3 与 18.8±9.7:p<0.01)上均有显著差异。
在先天性十二指肠疾病新生儿的术后喂养方案中,采用至少 2.5ml/kg 的口服或增量胃管喂养速度,分阶段逐步增加,每天多次喂养的初始喂养方案是完全可行的。这可使这些婴儿获得显著的健康益处,使他们能够更早地获得完全的肠内喂养并出院。