Moosa Muhammed Shiraz, Maartens Gary, Gunter Hannah, Allie Shaazia, Chughlay Mohamed F, Setshedi Mashiko, Wasserman Sean, Stead David F, Cohen Karen
Department of Medicine, New Somerset Hospital, Cape Town, South Africa.
Department of Medicine, Faculty of Health Sciences, University of Cape Town, Cape Town, South Africa.
South Afr J HIV Med. 2022 Jun 14;23(1):1376. doi: 10.4102/sajhivmed.v23i1.1376. eCollection 2022.
There are limited data on the outcomes of rechallenge with anti-tuberculosis therapy (ATT) following anti-tuberculosis drug-induced liver injury (AT-DILI) in a high HIV prevalence setting.
To describe the outcomes of rechallenge with first-line ATT.
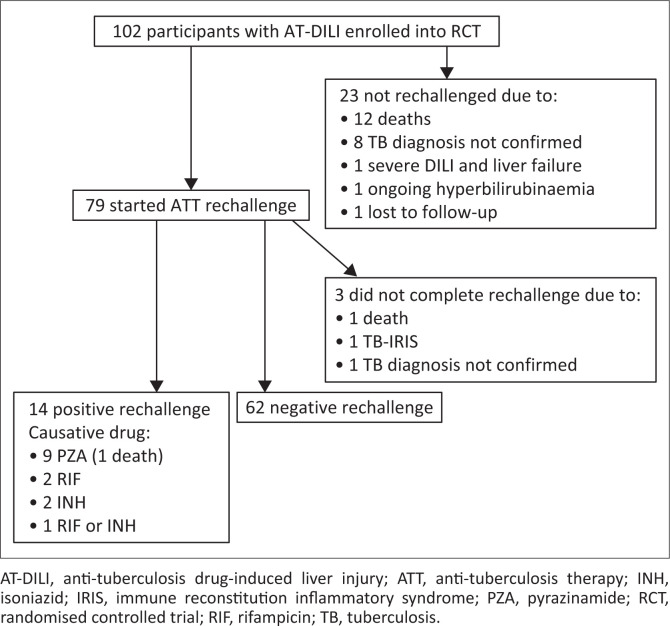
Hospitalised participants with AT-DILI who were enrolled into a randomised controlled trial of N-acetylcysteine in Cape Town, South Africa, were followed up until completion of ATT rechallenge. We described rechallenge outcomes, and identified associations with recurrence of liver injury on rechallenge (positive rechallenge).
Seventy-nine participants were rechallenged of whom 41 (52%) were female. Mean age was 37 years (standard deviation [s.d.] ±10). Sixty-eight (86%) were HIV-positive, of whom 34 (50%) were on antiretroviral therapy (ART) at time of AT-DILI presentation. Five participants had serious adverse reactions to an aminoglycoside included in the alternate ATT regimen given after first-line ATT interruption: acute kidney injury in three and hearing loss in two. The median time from first-line ATT interruption to start of first-line ATT rechallenge was 13 days (interquartile range [IQR]: 8-18 days). Antiretroviral therapy was interrupted for a median of 32 days (IQR: 17-58) among HIV-positive participants on ART before AT-DILI. Fourteen participants had positive rechallenge (18%). Positive rechallenge was associated with pyrazinamide rechallenge ( = 0.005), female sex ( = 0.039) and first episode of tuberculosis (TB) ( = 0.032).
Rechallenge was successful in most of our cohort. Pyrazinamide rechallenge should be carefully considered.
在艾滋病毒高流行地区,关于抗结核药物性肝损伤(AT-DILI)后重新使用抗结核治疗(ATT)的结果数据有限。
描述一线抗结核治疗重新使用的结果。
在南非开普敦,对纳入N-乙酰半胱氨酸随机对照试验的AT-DILI住院参与者进行随访,直至完成抗结核治疗重新使用。我们描述了重新使用的结果,并确定了与重新使用时肝损伤复发(阳性重新使用)的关联。
79名参与者接受了重新使用,其中41名(52%)为女性。平均年龄为37岁(标准差±10)。68名(86%)为艾滋病毒阳性,其中34名(50%)在出现AT-DILI时正在接受抗逆转录病毒治疗(ART)。5名参与者对一线抗结核治疗中断后给予的替代抗结核治疗方案中包含的氨基糖苷类药物有严重不良反应:3名出现急性肾损伤,2名出现听力损失。从一线抗结核治疗中断到一线抗结核治疗重新开始的中位时间为13天(四分位间距:8-18天)。在出现AT-DILI之前接受ART的艾滋病毒阳性参与者中,抗逆转录病毒治疗中断的中位时间为32天(四分位间距:17-58天)。14名参与者重新使用呈阳性(18%)。阳性重新使用与吡嗪酰胺重新使用(P = 0.005)、女性(P = 0.039)和首次发生结核病(TB)(P = 0.032)相关。
我们队列中的大多数重新使用是成功的。应仔细考虑吡嗪酰胺重新使用。