Ligtenberg Hans, Hackett Sara L, Merckel Laura G, Snoeren Louk, Kontaxis Charis, Zachiu Cornel, Bol Gijsbert H, Verhoeff Joost J C, Fast Martin F
Department of Radiotherapy, University Medical Center Utrecht, Heidelberglaan 100, Utrecht, The Netherlands.
Phys Imaging Radiat Oncol. 2022 May 24;23:24-31. doi: 10.1016/j.phro.2022.05.002. eCollection 2022 Jul.
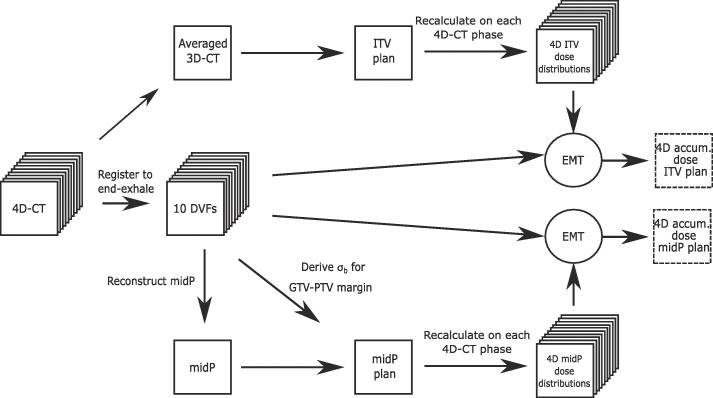
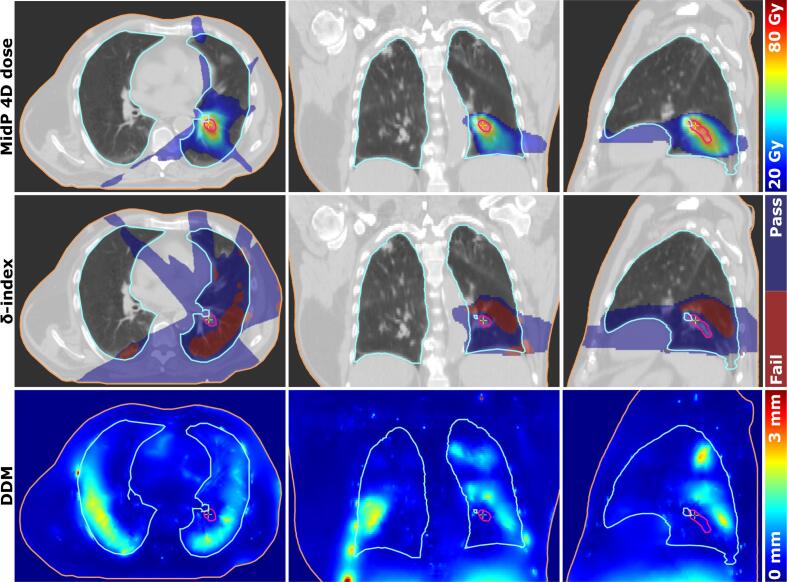
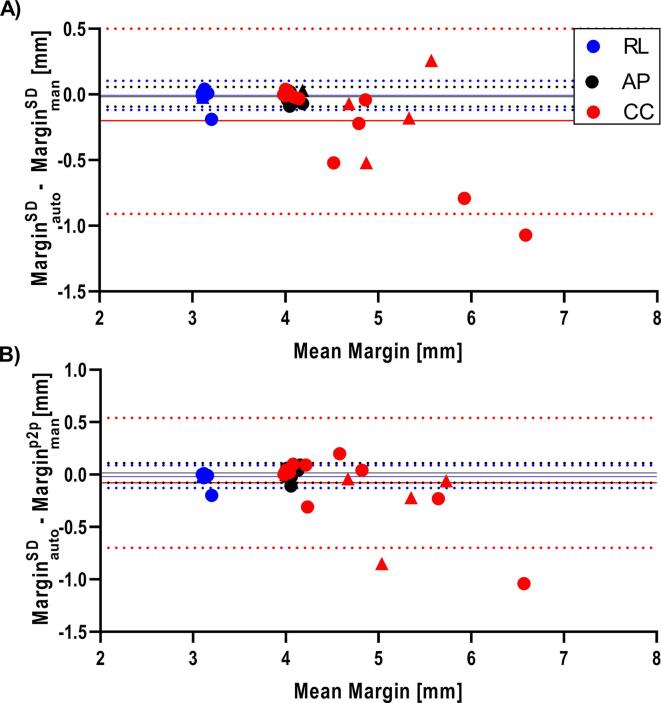
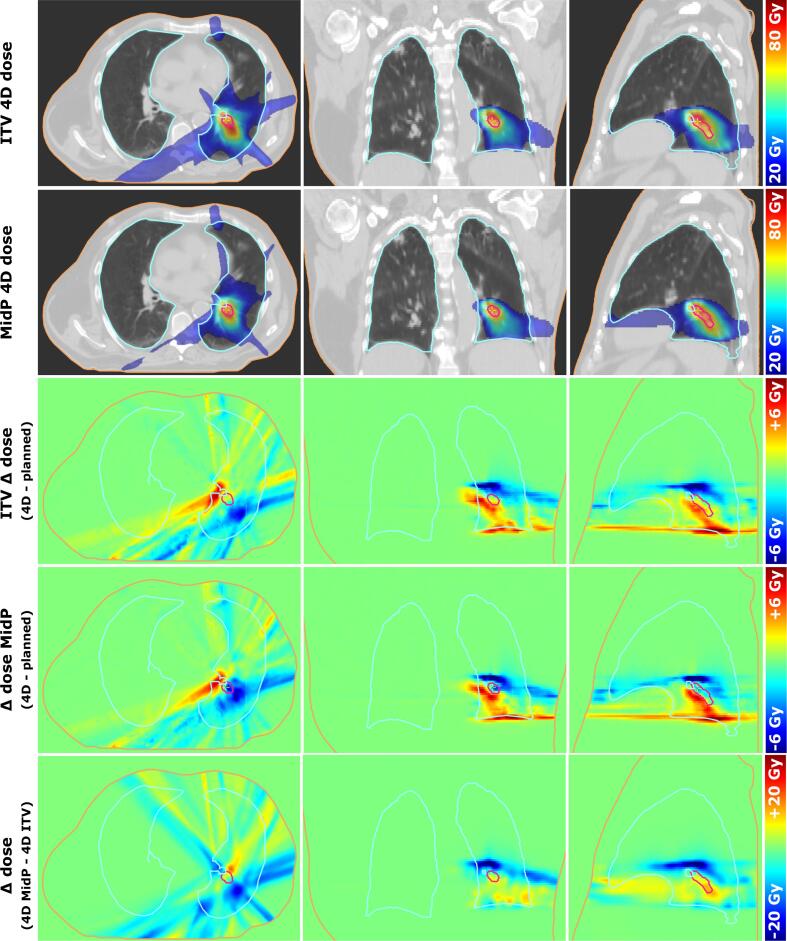
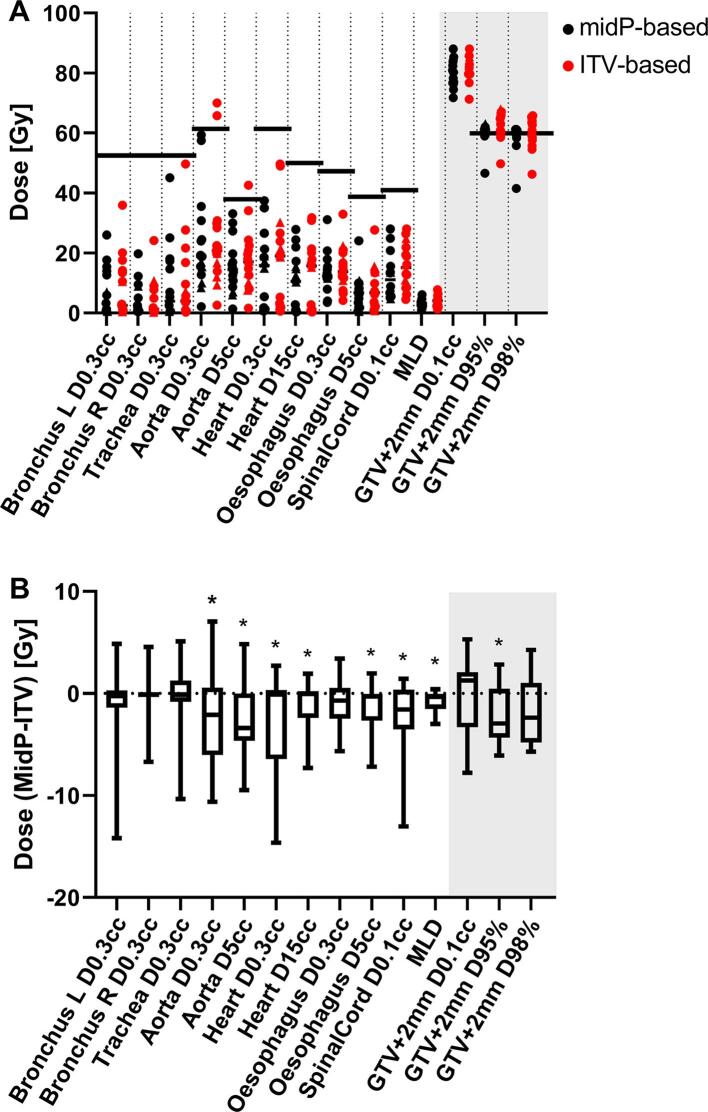
Central lung tumours can be treated by magnetic resonance (MR)-guided radiotherapy. Complications might be reduced by decreasing the Planning Target Volume (PTV) using mid-position (midP)-based planning instead of Internal Target Volume (ITV)-based planning. In this study, we aimed to verify a method to automatically derive patient-specific PTV margins for midP-based planning, and show dosimetric robustness of midP-based planning for a 1.5T MR-linac. Central(n = 12) and peripheral(n = 4) central lung tumour cases who received 8x7.5 Gy were included. A midP-image was reconstructed from ten phases of the 4D-Computed Tomography using deformable image registration. The Gross Tumor Volume (GTV) was delineated on the midP-image and the PTV margin was automatically calculated based on van Herk's margin recipe, treating the standard deviation of all Deformation Vector Fields, within the GTV, as random error component. Dosimetric robustness of midP-based planning for MR-linac using automatically derived margins was verified by 4D dose-accumulation. MidP-based plans were compared to ITV-based plans. Automatically derived margins were verified with manually derived margins. The mean D95% target coverage in GTV + 2 mm was 59.9 Gy and 62.0 Gy for midP- and ITV-based central lung plans, respectively. The mean lung dose was significantly lower for midP-based treatment plans (difference:-0.3 Gy; ). Automatically derived margins agreed within one millimeter with manually derived margins. : This retrospective study indicates that mid-position-based treatment plans for central lung Stereotactic Body Radiation Therapy yield lower OAR doses compared to ITV-based treatment plans on the MR-linac. Patient-specific GTV-to-PTV margins can be derived automatically and result in clinically acceptable target coverage.
中央型肺肿瘤可通过磁共振(MR)引导的放射治疗进行治疗。使用基于中位(midP)的计划而非基于内部靶区体积(ITV)的计划来减小计划靶区体积(PTV),可能会减少并发症。在本研究中,我们旨在验证一种为基于midP的计划自动推导患者特异性PTV边界的方法,并展示基于midP的计划在1.5T MR直线加速器上的剂量学稳健性。纳入了12例接受8×7.5 Gy的中央型肺肿瘤病例和4例周围型肺肿瘤病例。使用可变形图像配准从4D计算机断层扫描的十个时相重建midP图像。在midP图像上勾画大体肿瘤体积(GTV),并根据范·赫克边界公式自动计算PTV边界,将GTV内所有变形矢量场的标准差视为随机误差分量。通过4D剂量累积验证了使用自动推导边界的基于midP的MR直线加速器计划的剂量学稳健性。将基于midP的计划与基于ITV的计划进行比较。将自动推导的边界与手动推导的边界进行验证。对于基于midP和ITV的中央型肺计划,GTV + 2 mm处的平均D95%靶区覆盖率分别为59.9 Gy和62.0 Gy。基于midP的治疗计划的平均肺剂量显著更低(差异:-0.3 Gy; )。自动推导的边界与手动推导的边界在1毫米内一致。 :这项回顾性研究表明,与基于ITV的MR直线加速器治疗计划相比,基于中位的中央型肺立体定向体部放射治疗计划产生的危及器官剂量更低。可以自动推导患者特异性的GTV到PTV边界,并实现临床可接受的靶区覆盖率。