Arrichiello Gianluca, Pirozzi Mario, Facchini Bianca Arianna, Facchini Sergio, Paragliola Fernando, Nacca Valeria, Nicastro Antonella, Canciello Maria Anna, Orlando Adele, Caterino Marianna, Ciardiello Davide, Della Corte Carminia Maria, Fasano Morena, Napolitano Stefania, Troiani Teresa, Ciardiello Fortunato, Martini Giulia, Martinelli Erika
Oncology Unit, Department of Precision Medicine, Università degli Studi della Campania "Luigi Vanvitelli", Naples, Italy.
Oncology Unit, Casa Sollievo della Sofferenza Hospital, San Giovanni Rotondo, Italy.
Front Oncol. 2022 Jul 18;12:937114. doi: 10.3389/fonc.2022.937114. eCollection 2022.
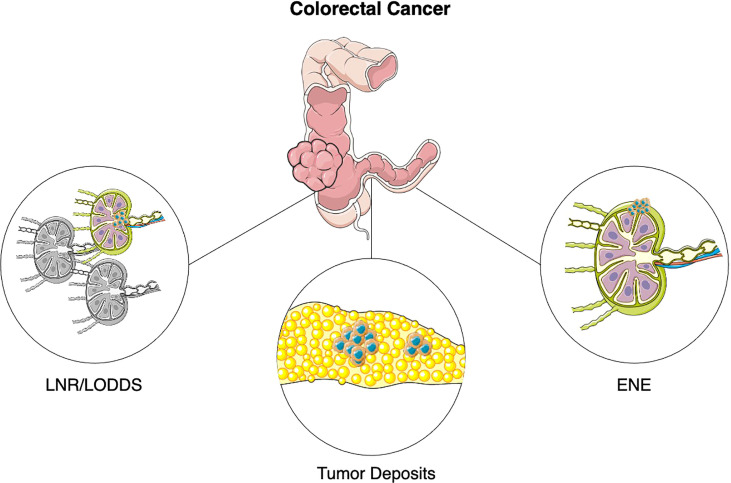
Traditionally, lymph node metastases (LNM) evaluation is essential to the staging of colon cancer patients according to the TNM (tumor-node-metastasis) system. However, in recent years evidence has accumulated regarding the role of emerging pathological features, which could significantly impact the prognosis of colorectal cancer patients. Lymph Node Ratio (LNR) and Log Odds of Positive Lymph Nodes (LODDS) have been shown to predict patients' prognosis more accurately than traditional nodal staging and it has been suggested that their implementation in existing classification could help stratify further patients with overlapping TNM stage. Tumor deposits (TD) are currently factored within the N1c category of the TNM classification in the absence of lymph node metastases. However, studies have shown that presence of TDs can affect patients' survival regardless of LNM. Moreover, evidence suggest that presence of TDs should not be evaluated as dichotomic but rather as a quantitative variable. Extranodal extension (ENE) has been shown to correlate with presence of other adverse prognostic features and to impact survival of colorectal cancer patients. In this review we will describe current staging systems and prognostic/predictive factors in colorectal cancer and elaborate on available evidence supporting the implementation of LNR/LODDS, TDs and ENE evaluation in existing classification to improve prognosis estimation and patient selection for adjuvant treatment.
传统上,根据TNM(肿瘤-淋巴结-转移)系统对结肠癌患者进行分期时,淋巴结转移(LNM)评估至关重要。然而,近年来,关于一些新出现的病理特征所起作用的证据不断积累,这些特征可能会显著影响结直肠癌患者的预后。淋巴结比率(LNR)和阳性淋巴结对数比值(LODDS)已被证明比传统的淋巴结分期能更准确地预测患者预后,并且有人提出在现有分类中采用它们有助于对TNM分期重叠的患者进一步分层。在无淋巴结转移的情况下,肿瘤结节(TD)目前被纳入TNM分类的N1c类别中。然而,研究表明,无论有无LNM,TD的存在都会影响患者的生存。此外,有证据表明,TD的存在不应作为二分变量来评估,而应作为一个定量变量。已证明结外扩展(ENE)与其他不良预后特征的存在相关,并会影响结直肠癌患者的生存。在本综述中,我们将描述结直肠癌目前的分期系统以及预后/预测因素,并详细阐述支持在现有分类中采用LNR/LODDS、TD和ENE评估以改善预后评估和辅助治疗患者选择的现有证据。