Program in Physical Therapy (C.E.L., C.L.H., G.M.E., K.R.L., M.D.B.) and Program in Occupational Therapy (C.E.L., M.D.B.), Washington University School of Medicine, St Louis, Missouri; Departments of Neurology (C.E.L., C.L.H., G.M.E., K.R.L., M.D.B.) and Neuroscience (G.M.E.), Washington University School of Medicine, St Louis, Missouri; Department of Brain and Psychological Sciences, Washington University, St Louis, Missouri (M.J.S.); Department of Physical Therapy, Boston University, Boston, Massachusetts (T.D.E., T.R.D., T.J.N.); Shirley Ryan Ability Lab, Chicago, Illinois (C.A.N., M.F.); and Department of Physical Therapy, University of Delaware, Newark (D.S.R.).
J Neurol Phys Ther. 2023 Jan 1;47(1):16-25. doi: 10.1097/NPT.0000000000000413. Epub 2022 Aug 4.
We addressed questions about the potential discrepancy between improvements in activity capacity and improvements in activity performance in daily life. We asked whether this discrepancy is: 1. Common in routine, outpatient care, or an artifact of intervention studies? 2. Unique to upper limb (UL) rehabilitation, or is it seen in walking rehabilitation too? 3. Only seen in persons with stroke, or a broader neurorehabilitation problem?
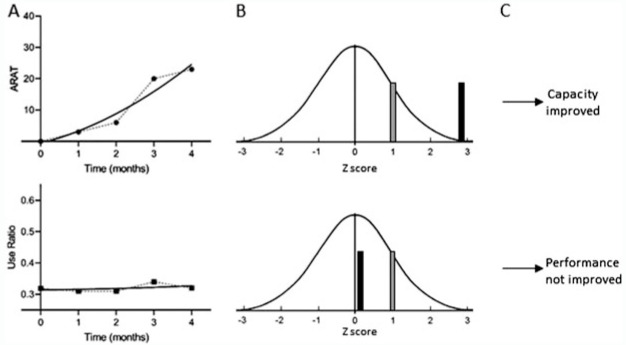
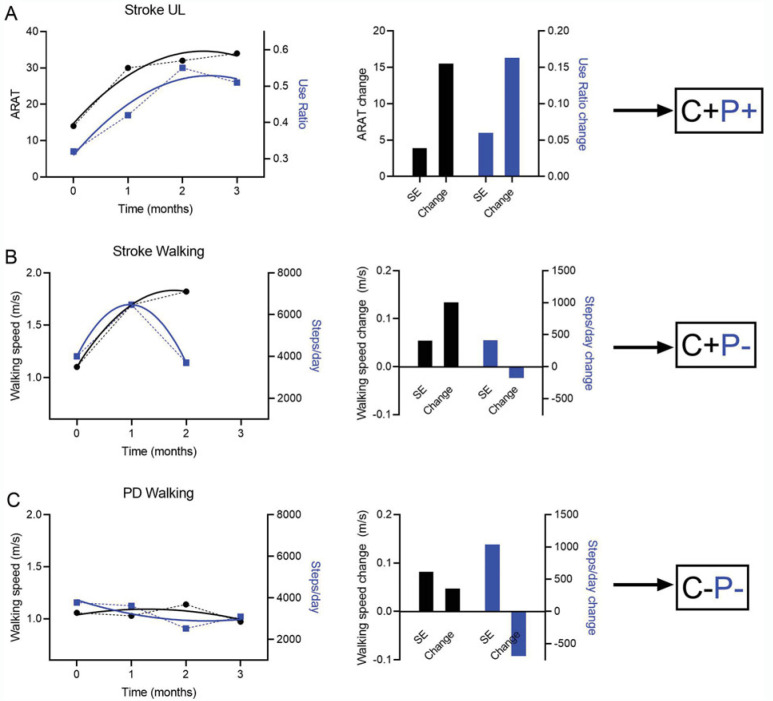
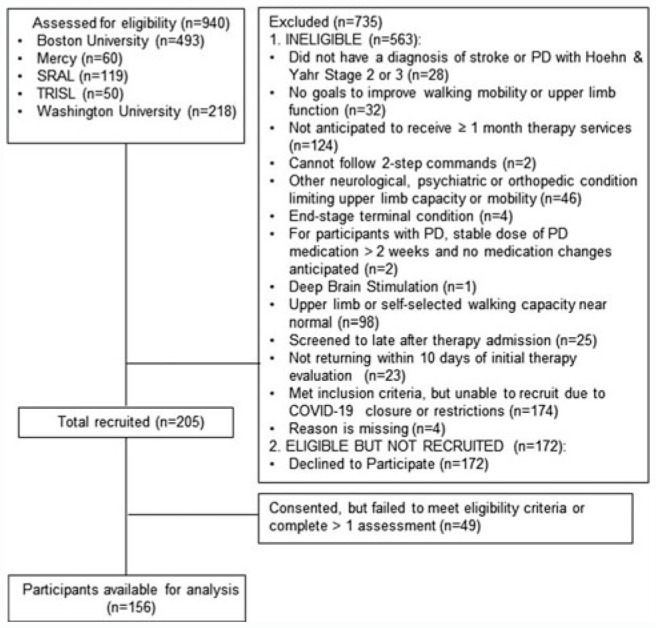
: A longitudinal, observational cohort of 156 participants with stroke or Parkinson disease (PD) receiving outpatient rehabilitation at 5 clinics was assessed around admission and monthly during their episode of care. Individual, longitudinal capacity (Action Research Arm Test or walking speed) and performance (wearable sensor measurements of use ratio or steps/day) data were modeled to extract predicted change scores. Simulation methods were used to determine whether an individual's change was greater than 1 standard error. Participants were classified into categories based on whether or not they improved in capacity (C+ or C−) and/or performance (P+ or P−).
: A majority (59%) were classified as C+P−. Smaller portions of the sample were classified as C+P+ (20%) and C−P− (21%), with 1 participant (<1%) classified as C−P+. The proportions in the C+P− category were significantly larger in the stroke (χ = 48.7, < 0.0001) and PD (χ = 24.3, < 0.0001) walking subgroups than in the stroke UL subgroup.
: The discrepancy between improvements in capacity and performance is a problem in routine, outpatient neurorehabilitation. If performance information were available, patients and clinicians could act to address it. for more insights from the authors (see the Video, Supplemental Digital Content 1, available at: http://links.lww.com/JNPT/A396).
我们探讨了在活动能力改善和日常生活中活动表现改善之间是否存在差异的问题。我们提出了以下三个问题:1. 这种差异在常规的门诊护理中是否常见,或者只是干预研究中的一个假象?2. 它仅见于上肢(UL)康复,还是也见于步行康复?3. 它仅见于脑卒中患者,还是更广泛的神经康复问题?
对 5 家诊所的 156 名脑卒中或帕金森病(PD)患者进行了一项纵向观察性队列研究,这些患者在入院时和接受门诊康复治疗期间每月接受评估。个体的纵向能力(行动研究上肢测试或步行速度)和表现(使用比例或每日步数的可穿戴传感器测量)数据被建模以提取预测的变化分数。使用模拟方法来确定个体的变化是否大于 1 个标准误差。根据患者在能力(C+或 C−)和/或表现(P+或 P−)方面是否有所改善,将患者分为不同的类别。
大多数(59%)患者被归类为 C+P−。较小比例的患者被归类为 C+P+(20%)和 C−P−(21%),1 名患者(<1%)被归类为 C−P+。在脑卒中(χ=48.7,<0.0001)和 PD(χ=24.3,<0.0001)步行亚组中,C+P−类别的比例明显大于脑卒中 UL 亚组。
在常规的门诊神经康复中,能力和表现改善之间的差异是一个问题。如果有表现信息,患者和临床医生可以采取行动来解决这个问题。[作者的更多观点,请观看视频,补充数字内容 1,可在以下网址获取:http://links.lww.com/JNPT/A396。]