Department of Pediatrics, Myunggok Medical Research Center, Konyang University College of Medicine, 158 Gwanjeodong-ro, Seo-gu, Daejeon, 35365, Korea.
Department of Pediatrics, Soonchunhyang University Cheonan Hospital, Sonnchunhyang 6-gil, Dongnam-gu, Cheonan, 31151, Korea.
BMC Pediatr. 2022 Aug 5;22(1):474. doi: 10.1186/s12887-022-03533-6.
This study aims to develop a new algorithm for predicting intravenous immunoglobulin (IVIG) resistance and coronary artery involvement in Kawasaki disease (KD) through decision tree models.
Medical records of children hospitalized for KD were analysed retrospectively. We compared the clinical characteristics, and the laboratory data in the groups with IVIG resistance and coronary artery dilatations (CADs) in KD patients. The decision tree models were developed to predict IVIG resistance and CADs.
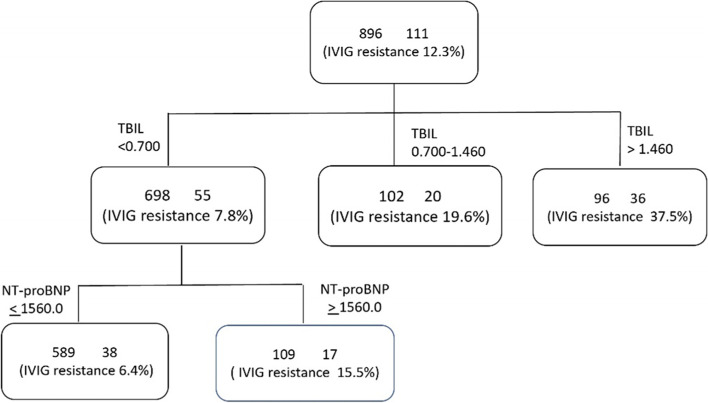
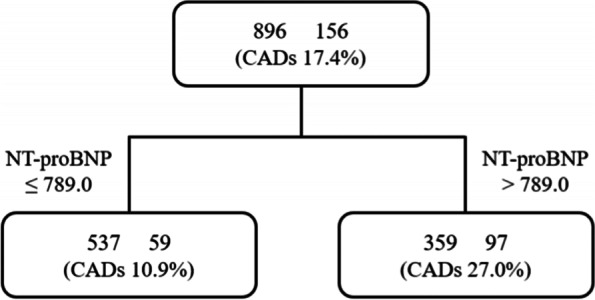
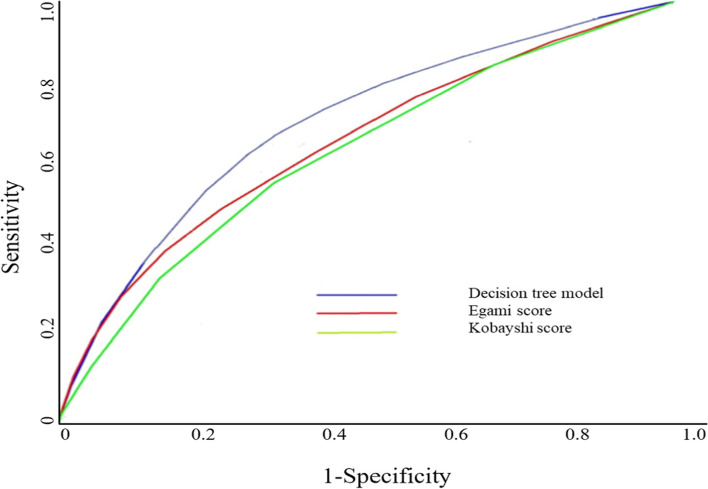
A total 896 patients (511 males and 385 females; 1 month-12 years) were eligible. IVIG resistance was identified in 111 (12.3%) patients, and CADs were found in 156 (17.4%). Total bilirubin and nitrogen terminal- pro-brain natriuretic peptide (NT-proBNP) were significantly higher in IVIG resistant group than in IVIG responsive group (0.62 ± 0.8 mg/dL vs 1.38 ± 1.4 mg/dL and 1231 ± 2136 pg/mL vs 2425 ± 4459 mL, respectively, P < 0.01). Also, CADs were more developed in the resistant group (39/111; 14.9% vs. 117/785; 35.1%, P < 0.01). The decision tree for predicting IVIG resistance was classified based on total bilirubin (0.7 mg/mL, 1.46 mg/dL) and NT-proBNP (1561 pg/mL), consisting of two layers and four nodes, with 86.2% training accuracy and 90.5% evaluation accuracy. The Receiver Operating Characteristic (ROC) evaluated the predictive ability of the decision tree, and the area under the curve (AUC) (0.834; 95% confidence interval, 0.675-0.973; P < 0.05) showed relatively higher accuracy. The group with CADs had significantly higher total bilirubin and NT-proBNP levels than the control group (0.64 ± 0.82 mg/dL vs 1.04 ± 1.14 mg/dL and 1192 ± 2049 pg/mL vs 2268 ± 4136 pg/mL, respectively, P < 0.01). The decision trees for predicting CADs were classified into two nodes based on NT-proBNP (789 pg/mL) alone, with 83.5% training accuracy and 90.3% evaluation accuracy.
A new algorithm decision tree model presents for predicting IVIG resistance and CADs in KD, confirming the usefulness of NT-proBNP as a predictor of KD.
本研究旨在通过决策树模型开发一种新的预测川崎病(KD)患者静脉注射免疫球蛋白(IVIG)耐药和冠状动脉受累的算法。
回顾性分析了因 KD 住院的儿童的病历。我们比较了 KD 患者中 IVIG 耐药组和冠状动脉扩张(CAD)组的临床特征和实验室数据。建立决策树模型以预测 IVIG 耐药和 CAD。
共有 896 名患者(男性 511 名,女性 385 名;年龄 1 个月至 12 岁)符合条件。111 名(12.3%)患者出现 IVIG 耐药,156 名(17.4%)患者出现 CAD。IVIG 耐药组的总胆红素和氨基末端脑利钠肽前体(NT-proBNP)明显高于 IVIG 反应组(0.62±0.8mg/dL 比 1.38±1.4mg/dL 和 1231±2136pg/mL 比 2425±4459pg/mL,均 P<0.01)。此外,耐药组的 CAD 更严重(39/111;14.9%比 117/785;35.1%,P<0.01)。用于预测 IVIG 耐药的决策树基于总胆红素(0.7mg/mL,1.46mg/dL)和 NT-proBNP(1561pg/mL)进行分类,由两层和四个节点组成,训练准确率为 86.2%,评估准确率为 90.5%。接受者操作特征(ROC)评估了决策树的预测能力,曲线下面积(AUC)(0.834;95%置信区间,0.675-0.973;P<0.05)显示出相对较高的准确性。CAD 组的总胆红素和 NT-proBNP 水平明显高于对照组(0.64±0.82mg/dL 比 1.04±1.14mg/dL 和 1192±2049pg/mL 比 2268±4136pg/mL,均 P<0.01)。用于预测 CAD 的决策树仅基于 NT-proBNP(789pg/mL)分为两个节点,训练准确率为 83.5%,评估准确率为 90.3%。
一种新的算法决策树模型可用于预测 KD 中的 IVIG 耐药和 CAD,证实了 NT-proBNP 作为 KD 预测因子的有用性。