Microbiology Unit, IRCCS Azienda Ospedaliero-Universitaria di Bologna, Bologna, Italy.
Pathology Unit, Azienda USL-IRCCS di Reggio Emilia, 42123, Reggio Emilia, Italy.
Cell Mol Neurobiol. 2023 Apr;43(3):1385-1399. doi: 10.1007/s10571-022-01258-9. Epub 2022 Aug 7.
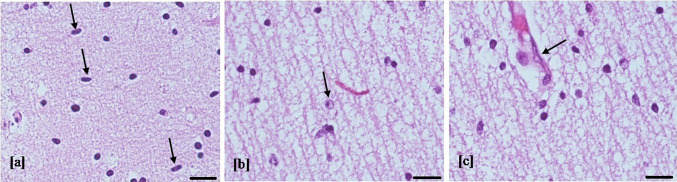
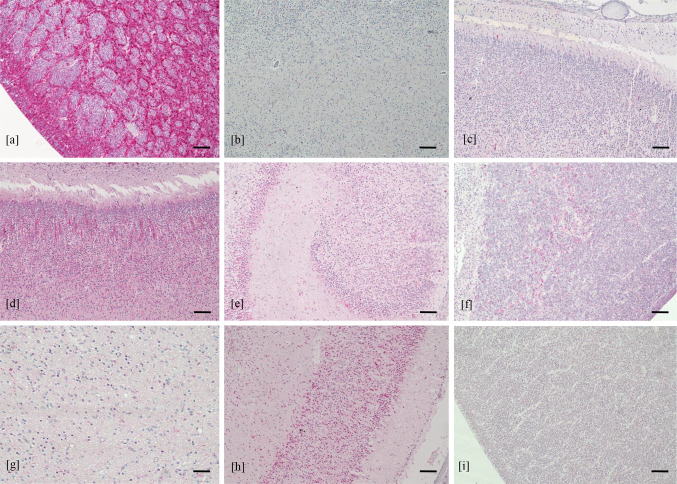
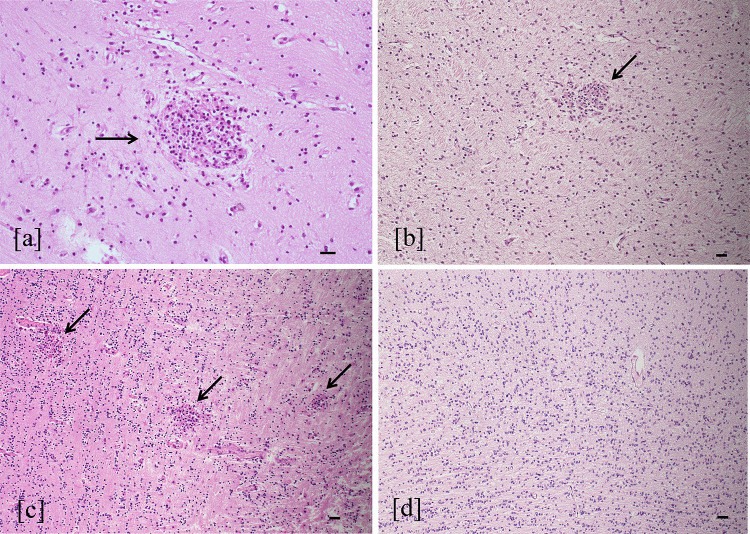
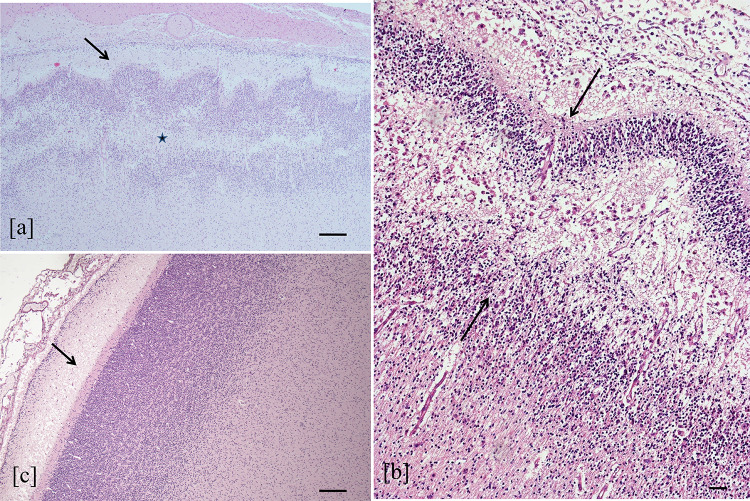
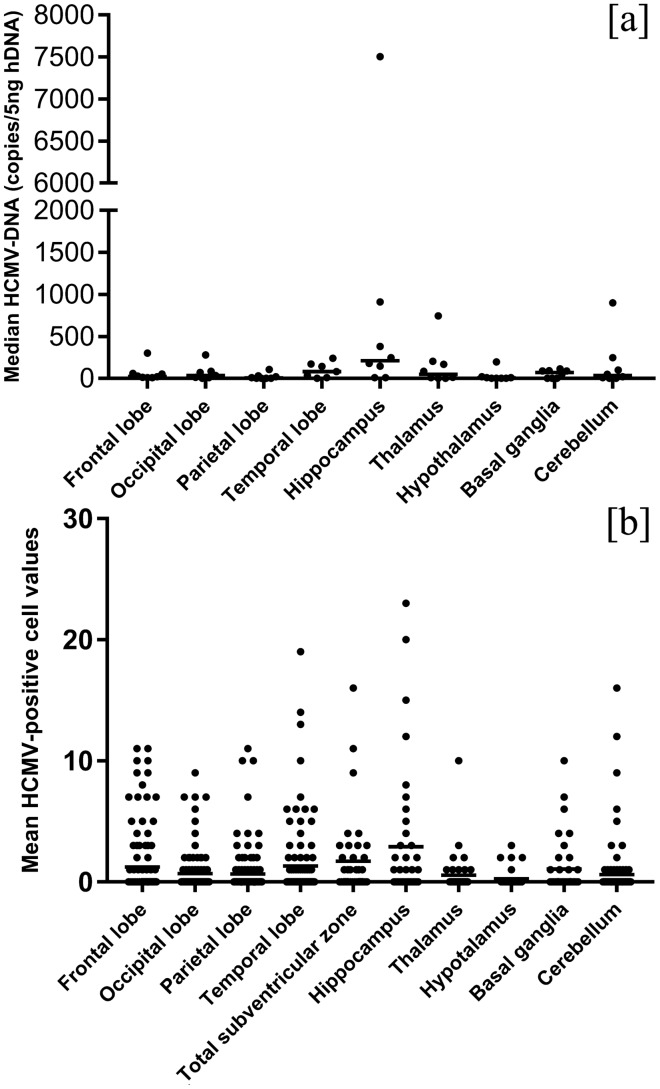
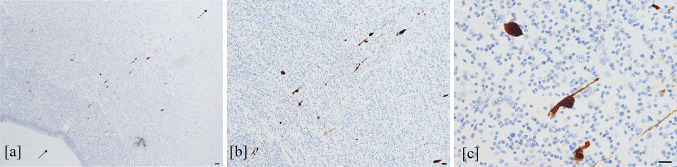
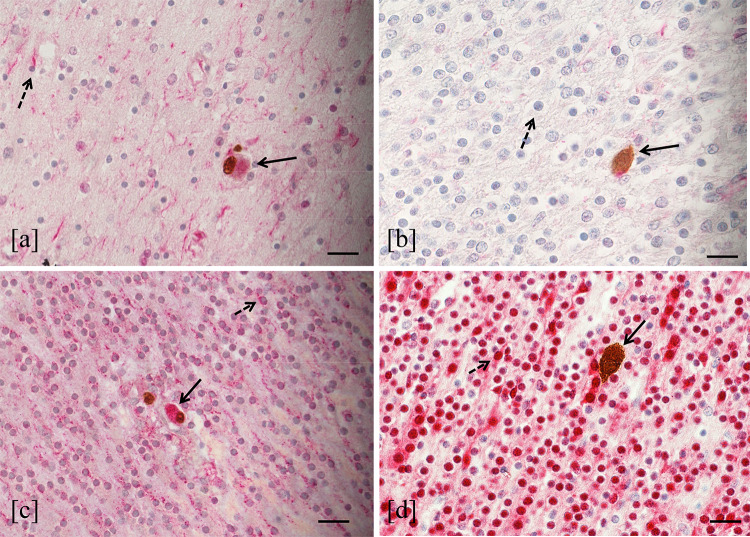
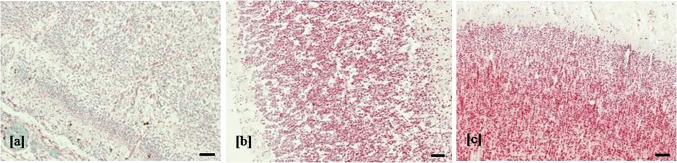
Human cytomegalovirus (HCMV) causes congenital neurological lifelong disabilities. To date, the neuropathogenesis of brain injury related to congenital HCMV (cCMV) infection is poorly understood. This study evaluates the characteristics and pathogenetic mechanisms of encephalic damage in cCMV infection. Ten HCMV-infected human fetuses at 21 weeks of gestation were examined. Specifically, tissues from different brain areas were analyzed by: (i) immunohistochemistry (IHC) to detect HCMV-infected cell distribution, (ii) hematoxylin-eosin staining to evaluate histological damage and (iii) real-time PCR to quantify tissue viral load (HCMV-DNA). The differentiation stage of HCMV-infected neural/neuronal cells was assessed by double IHC to detect simultaneously HCMV-antigens and neural/neuronal markers: nestin (a marker of neural stem/progenitor cells), doublecortin (DCX, marker of cells committed to the neuronal lineage) and neuronal nuclei (NeuN, identifying mature neurons). HCMV-positive cells and viral DNA were found in the brain of 8/10 (80%) fetuses. For these cases, brain damage was classified as mild (n = 4, 50%), moderate (n = 3, 37.5%) and severe (n = 1, 12.5%) based on presence and frequency of pathological findings (necrosis, microglial nodules, microglial activation, astrocytosis, and vascular changes). The highest median HCMV-DNA level was found in the hippocampus (212 copies/5 ng of human DNA [hDNA], range: 10-7,505) as well as the highest mean HCMV-infected cell value (2.9 cells, range: 0-23), followed by that detected in subventricular zone (1.7 cells, range: 0-19). These findings suggested a preferential viral tropism for both neural stem/progenitor cells and neuronal committed cells, residing in these regions, confirmed by the expression of DCX and nestin in 94% and 63.3% of HCMV-positive cells, respectively. NeuN was not found among HCMV-positive cells and was nearly absent in the brain with severe damage, suggesting HCMV does not infect mature neurons and immature neural/neuronal cells do not differentiate into neurons. This could lead to known structural and functional brain defects from cCMV infection.
人类巨细胞病毒(HCMV)可导致先天性神经发育障碍和终身残疾。迄今为止,先天性 HCMV(cCMV)感染相关的脑损伤的神经发病机制仍知之甚少。本研究评估了 cCMV 感染中脑损伤的特征和发病机制。对 21 周妊娠的 10 例 HCMV 感染的胎儿进行了检查。具体而言,通过以下方法分析不同脑区的组织:(i)免疫组织化学(IHC)检测 HCMV 感染细胞的分布,(ii)苏木精-伊红染色评估组织学损伤,(iii)实时 PCR 定量组织病毒载量(HCMV-DNA)。通过双重 IHC 评估 HCMV 感染的神经/神经元细胞的分化阶段,同时检测 HCMV 抗原和神经/神经元标志物:巢蛋白(神经干细胞/祖细胞标志物)、双皮质素(DCX,细胞向神经元谱系分化的标志物)和神经元核(NeuN,鉴定成熟神经元)。在 10 例胎儿中的 8 例(80%)的大脑中发现了 HCMV 阳性细胞和病毒 DNA。对于这些病例,根据病理发现(坏死、小胶质细胞结节、小胶质细胞活化、星形胶质细胞增生和血管改变)的存在和频率,将脑损伤分为轻度(n=4,50%)、中度(n=3,37.5%)和重度(n=1,12.5%)。在海马体(212 拷贝/5ng 人 DNA [hDNA],范围:10-7505)中发现最高的 HCMV-DNA 中位数,以及最高的 HCMV 感染细胞平均值(2.9 个细胞,范围:0-23),其次是在侧脑室下区(1.7 个细胞,范围:0-19)。这些发现表明病毒对这些区域中的神经干细胞/祖细胞和神经定向细胞具有优先的嗜性,这一点通过 HCMV 阳性细胞中分别 94%和 63.3%表达 DCX 和巢蛋白得到证实。在 HCMV 阳性细胞中未发现 NeuN,在严重损伤的大脑中几乎不存在,这表明 HCMV 不会感染成熟神经元,不成熟的神经/神经元细胞不会分化为神经元。这可能导致已知的先天性巨细胞病毒感染的结构性和功能性脑缺陷。